
The Lancet Lets it Lie
Lancet choose to ignore errors in paper on myocarditis in children


Dr Clare Craig
3 March 2026
Retractions are sometimes necessary, for example in cases of fraud, fabrication, or findings that are demonstrably unreliable, but the scientific record is not meant to be constantly rewritten. Progress normally occurs in a far more gradual way: hypotheses are proposed, results are reproduced or challenged, evidence accumulates, and conclusions slowly move closer to the truth.
In recent years, however, the retraction process itself has increasingly been used as a tool in scientific disputes. Papers have been removed not because their results were falsified, but because they were controversial or politically inconvenient. That is a worrying development. Science depends on open debate and reproducibility, not institutional gatekeeping.
For that reason, we are generally opposed to calls for retraction.
But occasionally the situation is different.
In the case of Sampri et al., “Vascular and inflammatory diseases after COVID-19 infection and vaccination in children and young people in England” (Lancet Child & Adolescent Health, 2025; 9:837–47), we concluded that a retraction request was warranted.
Not because the conclusion is controversial but because the analysis contains multiple structural problems that fundamentally undermine the headline claim. These include misrepresentation of crude incidence data, comparisons between non-comparable cohorts, instability in sensitivity analyses, and methodological decisions that systematically bias the results in one direction.
This matters because the paper has had substantial mainstream impact, in the UK and globally and was widely cited to support the claim that covid infection poses a greater myocarditis risk to children than vaccination.


When a paper with that level of influence contains major analytical problems, the responsibility on the journal to examine them carefully is particularly high.
For that reason, we submitted a detailed retraction request to the journal.
The response from The Lancet Child & Adolescent Health was a single sentence:
“Thank you for your email. We have discussed your request and find no grounds for further action.”
That was the entirety of the reply.
No explanation.
No engagement with the methodological concerns.
No indication that the evidence had been examined.
If this is the standard of scrutiny applied to challenges of influential papers, it raises a serious question about the role of major journals in maintaining the integrity of the scientific record.
Science should not depend on institutional authority.
It should depend on evidence.
The full retraction request is reproduced below so that readers can examine the arguments themselves.
To: Editor-in-Chief, The Lancet Child & Adolescent Health
Subject: Request for retraction — Sampri et al. (Lancet Child Adolesc Health 2025; 9:837–47)
Dear Editor,
I am writing to formally request the retraction of the article by Sampri et al., “Vascular and inflammatory diseases after COVID-19 infection and vaccination in children and young people in England”, published in The Lancet Child & Adolescent Health (2025; 9:837–47).
Substantial concerns about this paper have already been raised in several published letters, including my own, and those by Donzelli, Ulmer, and Saxena. These critiques cover multiple domains: misrepresentation of the crude incidence data, invalid comparison across non-aligned timeframes, implausible adjusted hazard ratios, reversal of conclusions in the study’s own sensitivity analyses, and the failure to stratify post-infection myocarditis risk by vaccination status. These omissions or misrepresentations in fact reverse the study’s headline conclusion.
The authors’ published reply acknowledges some of these issues, including a factual error in the main text regarding crude incidence rates, and the instability of key estimates in their sensitivity analysis. However, these admissions do not resolve the underlying problems. Instead, they confirm that the findings are not robust, and that the paper’s central conclusion rests on modelling that contradicts the unadjusted data, established epidemiological patterns, and the study’s own internal checks.
In summary, the paper’s headline claim — that covid infection poses a greater risk of myocarditis than vaccination in children — is not supported when the study’s own data, design choices, and sensitivity analyses are examined together. These are not minor or correctable errors: they systematically bias the results in one direction and meet the retraction criteria established by the Committee on Publication Ethics (COPE), including the presence of unreliable findings due to major errors, and conclusions no longer supported by the evidence presented. The detailed basis for this request is set out below.
Craig’s original letter challenged the figure of 650 admissions for myo/pericarditis over 27 months in the infection cohort shown in supplementary table S6, as implausibly large. Because this figure is restricted to events only from hospital admission records and ONS death records, it is one of the few data points in the paper that can be checked against the publicly available data which shows 226 admissions in those aged 0-17, over 24 months and 18 deaths over 3 full financial years. In their response, the authors firstly apologise for the figure being wrong and correct it to 425 and then explain the remaining disparity as being due to firstly differences in counting windows and secondly they introduced new information not stated in the paper, that the study population was not censored at age 18. This was unexpected as in multiple places the paper refers to the population studied as being younger than 18 years. There is therefore an additional confounder where a significant proportion of the myo/pericarditis counted in the study described as being in under 18 year olds was in fact in those aged 18 or over.
The authors acknowledge that around a third of the infection-attributed myocarditis cases may have been in people aged 18–20 despite describing the cohort repeatedly as 5–17 year-olds. The counting window difference between the 2 figures referred to is the 3 months from 1.1.2020 to 1.4.2020. If the average monthly rate over the other 24 months of the study is used to estimate the number of admissions during these 3 months, the extra admissions total about 28. Alternatively using the monthly average for the year April 2019-2020 the figure is about 29.5. If it is assumed the 18 deaths all occurred outside hospital and subtract 226+28+18 from 425, this leaves about 153 myo/pericarditis admissions in young people aged 18, 19 or 20 in the infection cohort. A different method using the number of person-years the average 18, 19 and 20 year old contributed to the study, as shown in table 2 below, gives a very similar estimate of 155 myocarditis or pericarditis admissions which includes about 72 aged 19 and about 2 aged 20 years.
Unfortunately as well as allowing those as old as 20 years to remain in the infection cohort, the failure to censor at age 18 introduces a new confounder, age, into the statistical analysis because of the unequal counting windows between infection and vaccine cohorts. The counting window for the infection cohort was 27 months whereas for the vaccine cohort it was 17 months. The infection cohort was therefore substantially older than the vaccine cohort. In table 3 below, the number aged 18-20 admitted with myo/pericarditis in the vaccine cohort is estimated to be 69, less than half of the number in the infection cohort. As the incidence of myocarditis is so age dependent this difference in age is critical. The 2 parts of this study consider such different populations over such different time periods, in both length and character, that they should be considered as 2 separate studies and not directly comparable.
But not only is this age group more likely to develop myocarditis or pericarditis, it is more likely to be vaccinated than those under 18 years old and more likely to be vaccinated during the infection cohort counting window and not during the vaccine cohort counting window. On 18th June 2021, the NHS sent 1.5 million texts to 18-20 year olds inviting them to make appointments for vaccination. Most of those taking up the offer would have received their vaccination during the infection cohort counting window and well before the start of the vaccine cohort counting window on 6th August 2021. As the study neither censored the infection cohort on vaccination or on reaching 18, this campaign alone will have significantly compromised the results and conclusions as is reflected in the study’s own sensitivity analysis, discussed in the next paragraph, which reverses the conclusions of the main analysis. These design features mean the cohorts are not structurally comparable, and therefore the study’s primary comparative analysis is not methodologically valid. The authors’ recommendations are untenable.
One of the study’s own sensitivity analyses – presented in appendix Table S16 but not addressed in the paper – separates the infection period into two phases and censors the infection cohort at the point of vaccination. For the period when vaccines were actually being offered to children (June 2021 to March 2022), the absolute excess risk of myocarditis and pericarditis following infection was 0.425 per 100,000. The excess risk following vaccination was 0.85 per 100,000 – twice as high. This reversal of the main conclusion is not mentioned in the main text and White’s letter raising this issue was not published. It undermines the core message of the study and has not been explained or corrected.
The direction of bias throughout the study is consistent. Key methodological decisions systematically inflated the risk of myocarditis attributed to infection and reduced the apparent risk after vaccination. A summary of these decisions is attached. Overall around three quarters of the cases after an infection would not have been included in a fair assessment.
These are not isolated or correctable flaws. The result is a paper whose headline claim — that COVID-19 infection poses a greater risk of myocarditis than vaccination in children — is not supported when examined against the full body of data in the study itself. That message has already been widely circulated and cited, including in public health contexts, based on an interpretation that misrepresented the crude data and omitted key limitations.
The necessary critiques have already been set out in the journal’s pages. The authors have had the opportunity to reply. The outcome of that exchange is clear: the corrected version of the paper remains unreliable, and its continued presence in the literature risks ongoing misunderstanding of vaccine safety in children.
I therefore respectfully ask that The Lancet Child & Adolescent Health initiate a formal retraction process in accordance with COPE guidelines.
Yours sincerely,
Dr Clare Craig, MBChB, FRCPath
APPENDIX
Decisions which inflated the incidence after infection and minimised the incidence post-vaccination
Including myocarditis and pericarditis events in individuals aged 18 to 20 while describing the study population as ages 5 to 17. Hospital admission data suggest that this design choice may account for one third or more of the included infection associated cases. The known age gradient in myocarditis risk makes this distortion particularly serious. Hospital Admitted Patient Care Activity data for the 4 years 2019-2020 to 2022-2023 suggest that the risk of admission due to myocarditis or pericarditis is about 10 times higher in the age group 18-19 than in the age group 0-17.
Defining the infection cohort as ages 0 to younger than 18 and the vaccine cohort as ages 5 to younger than 18. This allowed the inclusion of infants and toddlers in the infection group, who are more likely to be hospitalised for unrelated reasons and may meet myocarditis definitions as a secondary effect of other conditions.
Measuring infection associated risk from 1st January 2020 to 31st March 2022 while counting vaccine associated risk only from 6th August 2021 to 31st December 2022. This allowed early periods with more severe viral effects to influence the infection estimate while limiting the vaccine estimate to later phases when circulating variants were milder.
Failing to censor the infection cohort at the point of vaccination. This resulted in vaccine related myocarditis events being attributed to infection.
Not stratifying infection associated risk by vaccination status. This prevented analysis of whether vaccination increases total myocarditis risk when infection occurs.
Excluding individuals aged 19 to 24 from the vaccine analysis despite describing the population as children and young people. These older adolescents and young adults received the same vaccines, often at higher doses, and have shown consistently higher rates of myocarditis.
Reporting pooled rates that combine hospitalised and non hospitalised cases without clear separation. Sensitivity analyses limited to hospitalised cases produced materially different results that were not reflected in the headline conclusions.
Applying multiple layers of statistical adjustment that produced age and sex risk patterns inconsistent with wider epidemiological evidence. The analysis did not show higher myocarditis risk in male adolescents and instead showed higher estimated risk in younger children. These inconsistencies were presented without explanation or qualification.
Each of these decisions independently introduces distortion. Taken together they render the headline conclusion unreliable.
Table 1: Summary of major confounders in the paper
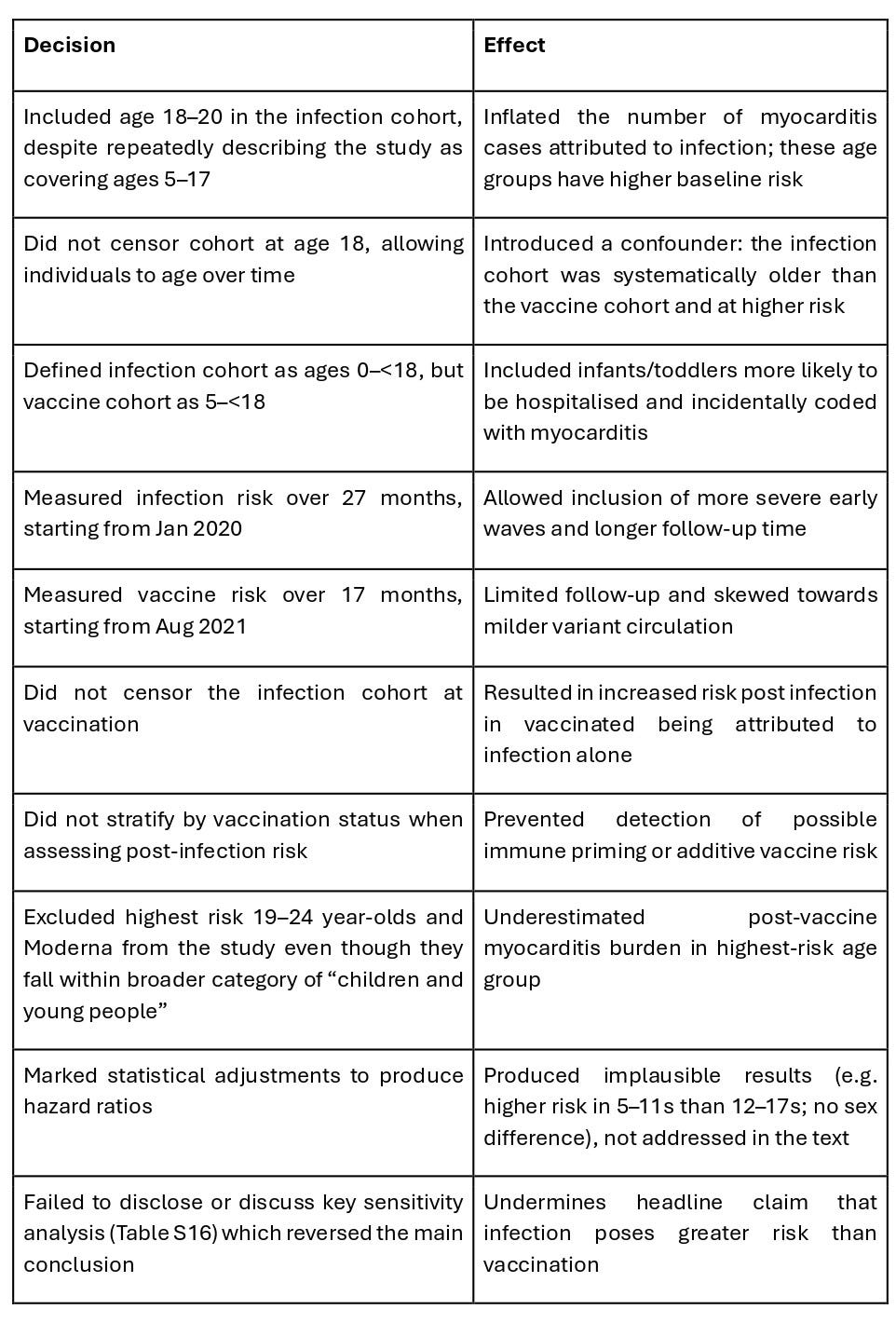
Table 2: Infection cohort. Estimated number of myocarditis/pericarditis admissions aged 18-20 years, during study follow-up, as a result of failure to censor at age 18, accounting for age-specific person-years of observation.
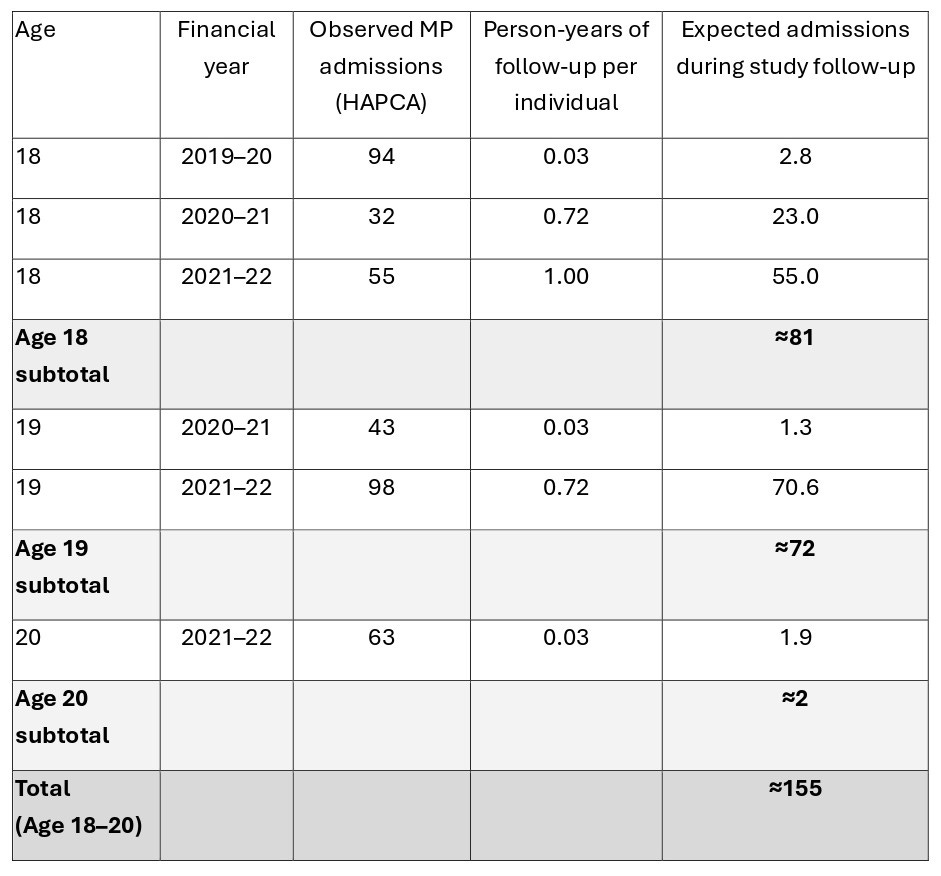
Notes:
Person-years represent the average follow-up per individual in each single-year age band, accounting for absence of censoring at age 18.
Expected admissions were calculated as observed NHS Hospital Admitted Patient Care Activity counts multiplied by the corresponding person-year fraction.
Financial years run from 1 April to 31 March.
Table 3: Vaccination cohort. Estimated number of myocarditis/pericarditis admissions aged 18 and 19 years, during study follow-up, as a result of failure to censor at age 18, accounting for age-specific person-years of observation.
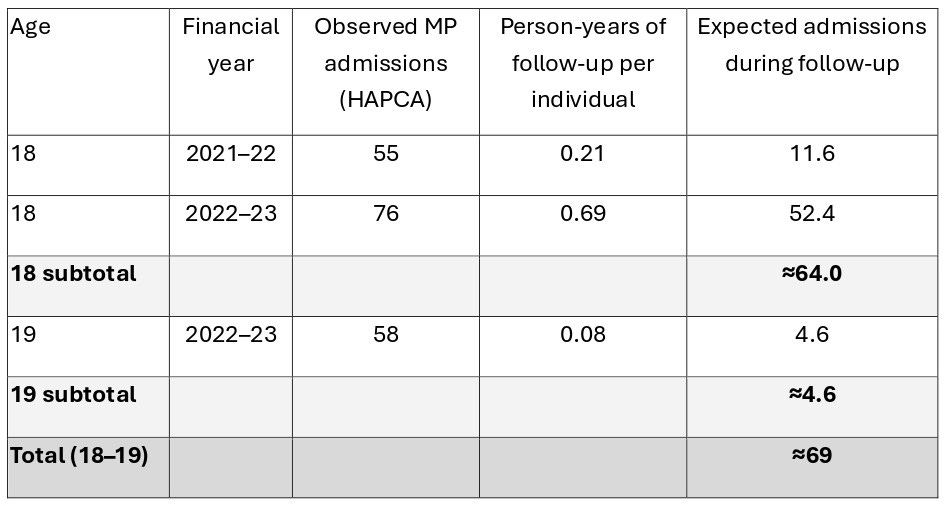
Notes:
Because the vaccine cohort counting window was 10 months shorter than the infection cohort counting window (17 months v 27 months) there were no 20 year olds in the vaccine cohort.
"No explanation.
No engagement with the methodological concerns.
No indication that the evidence had been examined."
Sadly it looks like the Lancet is treating your request for retraction with considered contempt. I wish you could send this request for retraction to every doctors surgery and doctor in the UK. Many who still believe they the Lancet are impartial
It looks like the Lancet is moving away from scientific rigour and in consequence the truth. They have done a risk assessment and decided the damage to their reputation by ignoring you is not sufficient to justify a meaningful response.
It makes you wonder about everything else they publish. If I were a doctor I would start looking sideways at everything this bunch put out.
Diagnosis... Compromised.
'Unreliable' .... wowsers. And this is our kids, our future's health. If only the MSM had 1% of your guts and integrity to speak up. Thank you for all your efforts.