




The account below was sent in to us by a HART follower who works in a busy A&E department, comparing the workload and the treatment options in the spring of 2020 with that of 2024. Here we reproduce it in full, with some added links to previous HART articles.
“I have always wondered about the ‘noticing’ of what became known as SARS-COV-2 in April 2020. Of course, evidence shows it was circulating for a long time before that, and that the response (in my opinion) was worse than the disease for the overwhelming majority of humans on the globe. But I did see sick people that spring/summer (and a small minority of very sick) and always wondered why the ‘peak’ was then and not over the winter. The views range from there being no such thing as a virus, there being no novel virus, there being an out of season virus, there being a virus which was lethal because of the response, there being a weaponised virus, through to (the least likely) that there was an easily spread killer virus which ‘the vaccine’ saved us from. Apologies if I have left out an obvious category, and I accept that combinations of the above form other views. I have a view, but that’s not a point I’m trying to push here.
What I did notice, was that when I slowed down over last weekend from a heavy, sustained workload, and the sun appeared for the first time — when I retired from rotavating the garden — I got sick with an upper respiratory tract illness — you know the type — pounding headache, dripping sinuses, copious catarrh, painful cough and (the worst bit) agony when you laugh. Having not slept for two nights, I ignored the advice of my better half and headed for work at 7am, only to take calls from a plethora of trainees who had decided not to show for their shifts because they were smitten with ‘feeling poorly’, ‘coughs’ etc — the most spectacular one being an e-mail that they could not come in because ‘they were absent’ (and not in the seizure sense). One industrious trainee had managed to score an NHS swab as positive for influenza B. I make no claim to martyr status for going in (nobody would listen in our place anyway) but it did strike me that among staff and patients there is widespread upper respiratory tract illness. And it is April.
For those with COPD, obesity, advanced years, polypharmacy, from institutions, immunocompromised etc — it is no surprise that they are getting superimposed bacterial lower respiratory tract infections… some even breaking through to ‘sepsis’. Thing is, I am no longer prohibited from admitting these patients and my treatment options extend beyond paracetamol, oxygen and ICU. We have regressed back into atrocious, antiquated treatment modalities like antibiotics, non-invasive ventilatory support, nebulisers, corticosteroids. I can talk to them without PPE, they can have direct contact in nursing care, the chest physios are back in action, and their relatives can be there for support. “Sepsis Six” is back in favour (thank you Ron Daniels) and we can resuscitate in the Resuscitation Room. (OK, I exaggerate, we are overwhelmed and today we treated 10 admissions in ambulances and 60 in the corridors; some into their third day. But you get the gist).
Did I mention — it is April? I don’t know how I have practised Emergency Medicine for over 30 years and not noticed the spring/summer (viral?) URTI/LRTI ‘waves’. Maybe because all-cause mortality has a seasonal (dark, cold, sunless) winter spike — but it is real in other seasons too.
And I feel really lousy; but better equipped to rationalise the madness of April 2020. Take my current condition, add two or three morbidities, reduce therapeutic options and pile on the FEAR — or even my current condition with just the FEAR (friends were sending me Ivermectin from India back then) and I think my condition today would not be that different from 2020.”
For those readers who like some charts, these from 2009 show that when there is a stated ‘pandemic’ and lots of ‘testing’, spring and summer waves are easily demonstrated…
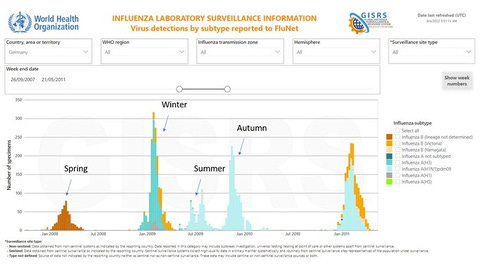



As the account above highlights, filling the population with FEAR and telling people to stay at home, avoid their general practitioner and only go to hospital when they are blue or breathless at rest, then banning their relatives, dressing all the staff in military PPE and doing a PCR test to demonstrate a ‘novel’ and dangerous pathogen which then directs the patient to a no-antibiotics, no-steroids protocol, quite easily transforms a ‘summer cold’ into a life-threatening condition. That is without the DNR notices and the Midazolam.
Reading between the lines, based on the evidence presented here, I think the conclusion must be that "SARS-CoV-2" was not a "novel", "deadly" virus then? One can accept that it exists and even that it is sufficiently genetically distinct to be uniquely characterised as a virus without admitting that it caused a novel disease (COVID) for which there was no suitable, existing treatment. Because that seems to be the most plausible explanation right now. In that case, one must conclude that all the death was due to something else, some of which has been mentioned here - denial of regular treatment in the presentation of ILI symptoms, misuse of other treatments, disruption to the general fabric of social and medical welfare... The response was responsible for all the excess death, not a novel virus.
I learned today that conundra is an acceptable plural for conundrum - and that's what it seems we have here with trying to piece together what was *actually* going on with respect to The Great Cough of Catastrophe™ known as 'covid'.
On the one hand we have the diagnostic testimony of Pierre Kory who argues that we were indeed dealing with a virus that was novel enough to be able to come to a different diagnosis. Furthermore, he argues that 'standard' treatments one would apply for serious ILI type illnesses did not work as well as expected, which is why he (and others) developed an alternative protocol. His diagnostic sentiments were also echoed by the doctor who treated my brother when he was hospitalized for covid complications. He also didn't know how best to treat his patients.
Another member of my family is an ICU nurse who treated the seriously ill during covid and she gets quite cross when people suggest it was 'non-existent' or just a misdiagnosed 'normal' virus. Do we ignore the testimony of those who were at the sharp end dealing with some very ill people?
On the other hand we have the kind of testimony of today's post above which demonstrates a wholly inadequate protocol was imposed in the UK (I presume) and this *must* have significantly contributed to the death toll - assuming we were dealing with a viral respiratory infection.
But this is the material fact isn't it? We must explain why people were getting ill. Was this unusual for this time of the year? Did we see a higher incidence of illness in age groups we wouldn't normally expect to see it in?
This is probably where I'd look for evidence for the hypothesis there was a novel-enough virus doing the rounds. Did we see an atypical incidence of hospital admissions for respiratory conditions in, say, the 20-40 year age range? Or even 40-60, for example? I don't know where to get that data.
I did a 'back of the envelope' calculation of the excess death as a percentage of the 2015-2019 baseline broken down into age ranges using the ONS data, and it showed that, when expressed as a percentage, there were noticeable 'spikes' during 'covid' waves across all except the very youngest age ranges.
But, but, but . . . (a) it's death by registration date data and (b) it's using the most crude estimate of excess of a simple arithmetic mean. And confidence intervals and error bars? Well, let's just say they were nowhere to be seen! So my back of the envelope methodology is providing only a *hint* at a possible problem.
If you look at the data from OWID (which we now know to be highly questionable and based to some extent on computed models) we also see another curious thing during the first year. There's a geographic pattern to covid death in Europe. Certain countries get hit with a wave in the Spring, but other countries in more central Europe have very little covid death in the Spring and then massive rises in the Winter. Did their treatment protocols change in this period?
If we're going to argue that much of the death was caused by (a) panic brought on by the announcement of a pandemic and (b) hopelessly inadequate treatment protocols (not to mention overuse of midazolam) then what explains the 'delay' in deaths in central European countries?
It's all a big mess - and a large part of the confusion must be placed at the door of the 'data' collection which seemed to me to be wholly unsuitable for the job. Who in their right mind, in the midst of a supposedly deadly 'pandemic', would insist on anything but the absolute most careful and accurate data collection? We spent billions on useless shite like testing and tracking but couldn't invest in decent data collection? The breath-taking stupidity of designating anyone who died within 4 weeks of a positive covid test as a 'covid' death is still something I have not been able to get my head round (from a scientific perspective. As a propaganda tool it makes perfect sense)
Anyway, there's still a lot about the whole covid clownshow that I can't make full sense of. At the moment I tend to think that (a) there was a novel-enough virus doing the rounds that (b) a very large portion of the deaths were essentially iatrogenic and that (c) the 'pandemic', such as it was, came nowhere close enough to justify the crazy levels of panic and idiotic interventions we suffered.