
The great disruption
Lockdowns, healthcare disruption and excess deaths from gallstones.

Dr David White
The first lockdown began on Monday 23rd March 2020 and was rapidly implemented in response to the emerging situation. Following this, the number of emergency hospital admissions for acute cholecystitis, cholecystectomy operations, and bile duct procedures fell substantially. These reductions were followed by a rise in deaths from gallstone disease.
Gallstones are not known to be caused by Covid-19, making it a good control case for estimating harm from policy. The temporal relationship, magnitude of service disruption, and the known natural history of gallstone disease together suggest that healthcare disruption was a major contributing factor in these excess deaths.
This raises important questions: what was the nature and scale of the disruption, and have services and patient outcomes recovered, or are we still dealing with the consequences six years on?
Key points:
Lockdowns disrupted NHS services on a massive scale: about 55,479 fewer cholecystectomy operations and 18,027 fewer endoscopic bile duct procedures over five years.That level of disruption likely killed people: approximately 575 excess deaths from gallstone and gallbladder disease followed, rising year on year and still not resolved.Gallstone disease is an ideal control: it has no known link to Covid-19, making these excess deaths a clean signal of policy harm rather than viral harm.Six years on, neither services nor outcomes have recovered — operations remain tens of thousands below baseline, and gallstone deaths in 2024 were 23% above projected levels.The true toll is almost certainly undercounted: loose death certification guidance created conditions in which untreated gallbladder deaths could plausibly have been registered as Covid-19.If a single surgical condition accounts for 575 preventable deaths, gallbladder disease is likely a small window onto a much larger and still unacknowledged catastrophe of indirect harm.
First it helps to know some basic anatomy and a little terminology (more explanation in this NHS leaflet).
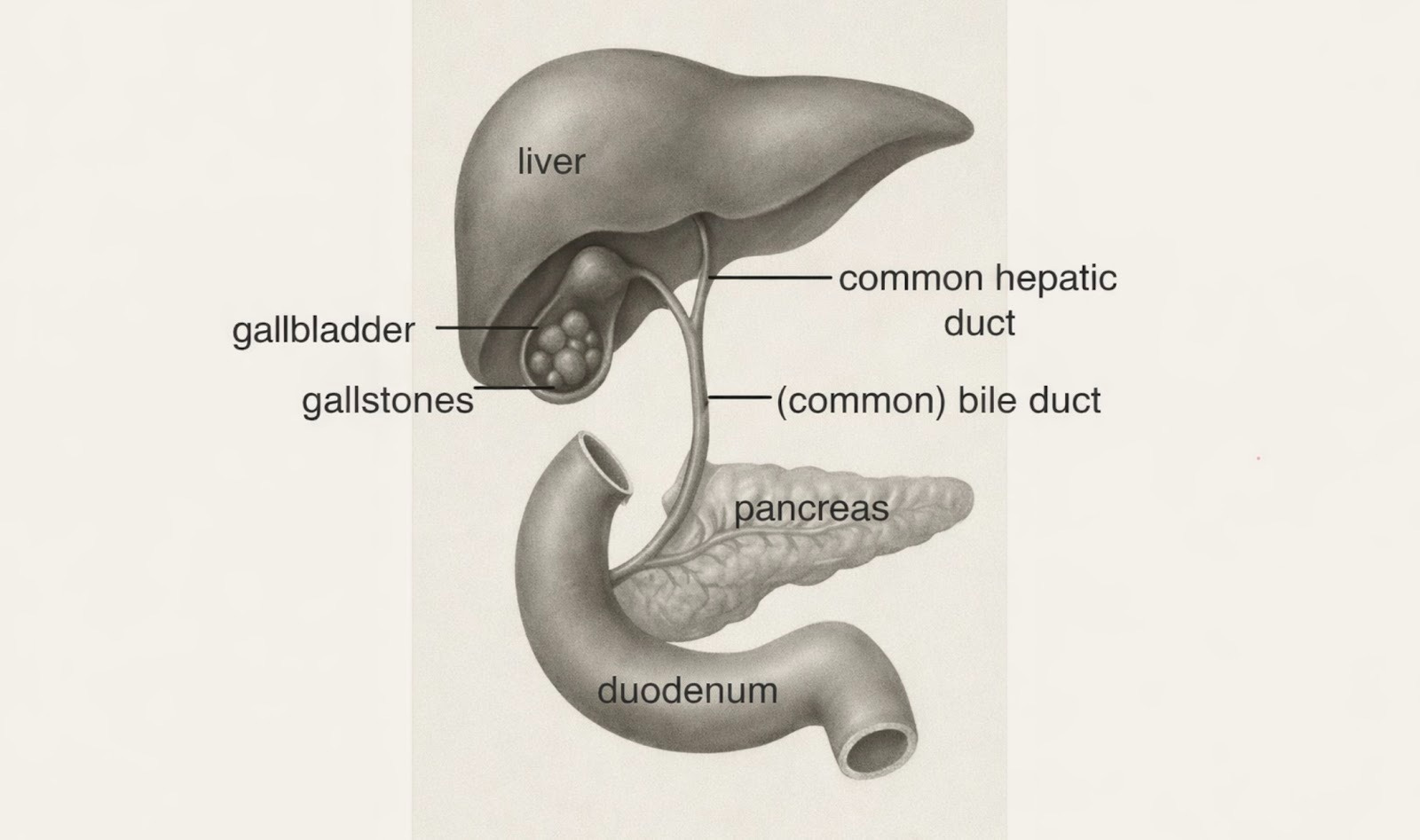
Figure 1. Bile is produced by the liver, stored in the gallbladder and discharged into the intestine mixed with pancreatic juices to help fat digestion.
Some medical terminology
Gallstones - small stones that form in the gallbladder in about 15% of people.
Cholelithiasis - the formation of or presence of gallstones. Cholelithiasis can be the underlying cause of death for statistical purposes.
Gallbladder - a small, pear-shaped organ located under the liver that stores and concentrates bile, a digestive fluid made by the liver that helps break down fats. When you eat fatty foods, the gallbladder contracts and releases bile into the intestine to aid digestion. Humans and mice have gallbladders but rats do not.
Cholecystitis - inflammation of the gallbladder. A common cause of emergency hospital admission, usually associated with gallstones and usually followed by a cholecystectomy operation.
Cholecystectomy or excision of gallbladder - removal of gallbladder operation often done after an attack of cholecystitis, mostly by laparoscopic or keyhole surgery.
Biliary tract - normally includes the gallbladder and associated ducts that transport bile from the liver to the duodenum (the first part of the intestine).
Cholangitis - a life-threatening infection which spreads along the bile duct to the liver, usually caused by blockage of the bile duct due to a stone which originated in the gallbladder.
Pancreatitis - inflammation of the pancreas, which may be acute or chronic and maybe related to gall stones or to alcohol or other toxins or to certain infections (K85-86).
ICD-10 (International Classification of Diseases, 10th revision) considers the gallbladder separately from the rest of the biliary tract. Below, the term gallbladder disease refers to ICD-10 categories - K81 cholecystitis, and K82 other diseases of the gallbladder. K80 cholelithiasis or gallstones, includes stones in the gallbladder (about 85%) and stones in the bile duct (about 15%). Gallbladder malignancies are not included in these deaths and are classified in ICD-10’s C category.
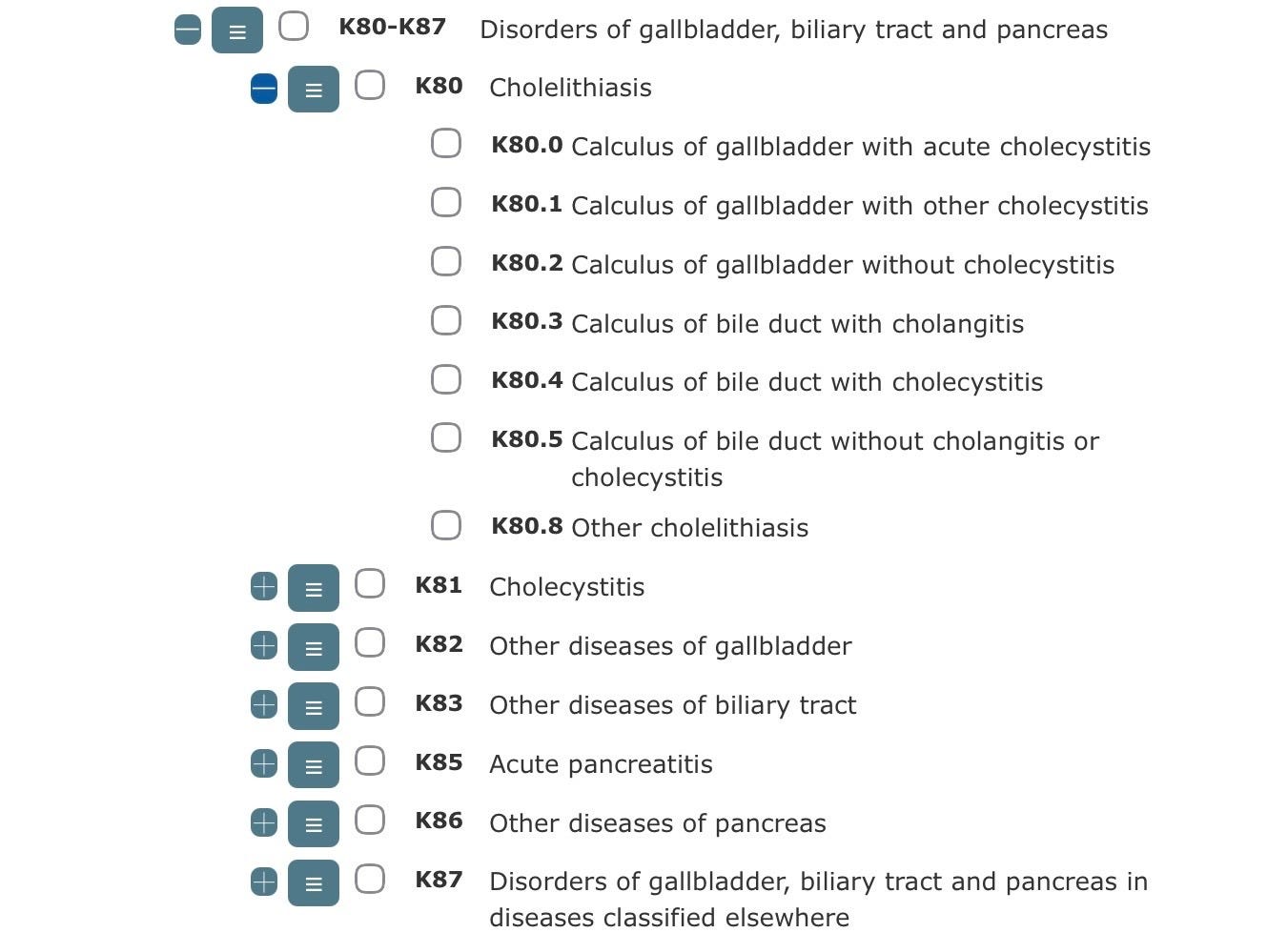
Figure 2. Extract from ONS nomis showing how ICD-10 categories break down into 3 and 4 character ICD-10 codes.
The increase in gallbladder disease and related deaths.
Cause of death data for England and Wales since 2013, are publicly available on the UK government’s nomis website which is run by the Office for National Statistics (ONS). The underlying cause of death is taken from the death certificate and matched to an ICD-10 code. The graph below (figure 3) shows gallbladder, biliary tract and pancreatic disease deaths. These are all of the deaths in ICD-10’s K-category. Deaths have increased at a higher rate since 2020.
Figure 3. England and Wales, gallbladder, biliary tract and pancreatic disease deaths (K80-87), ONS nomis.
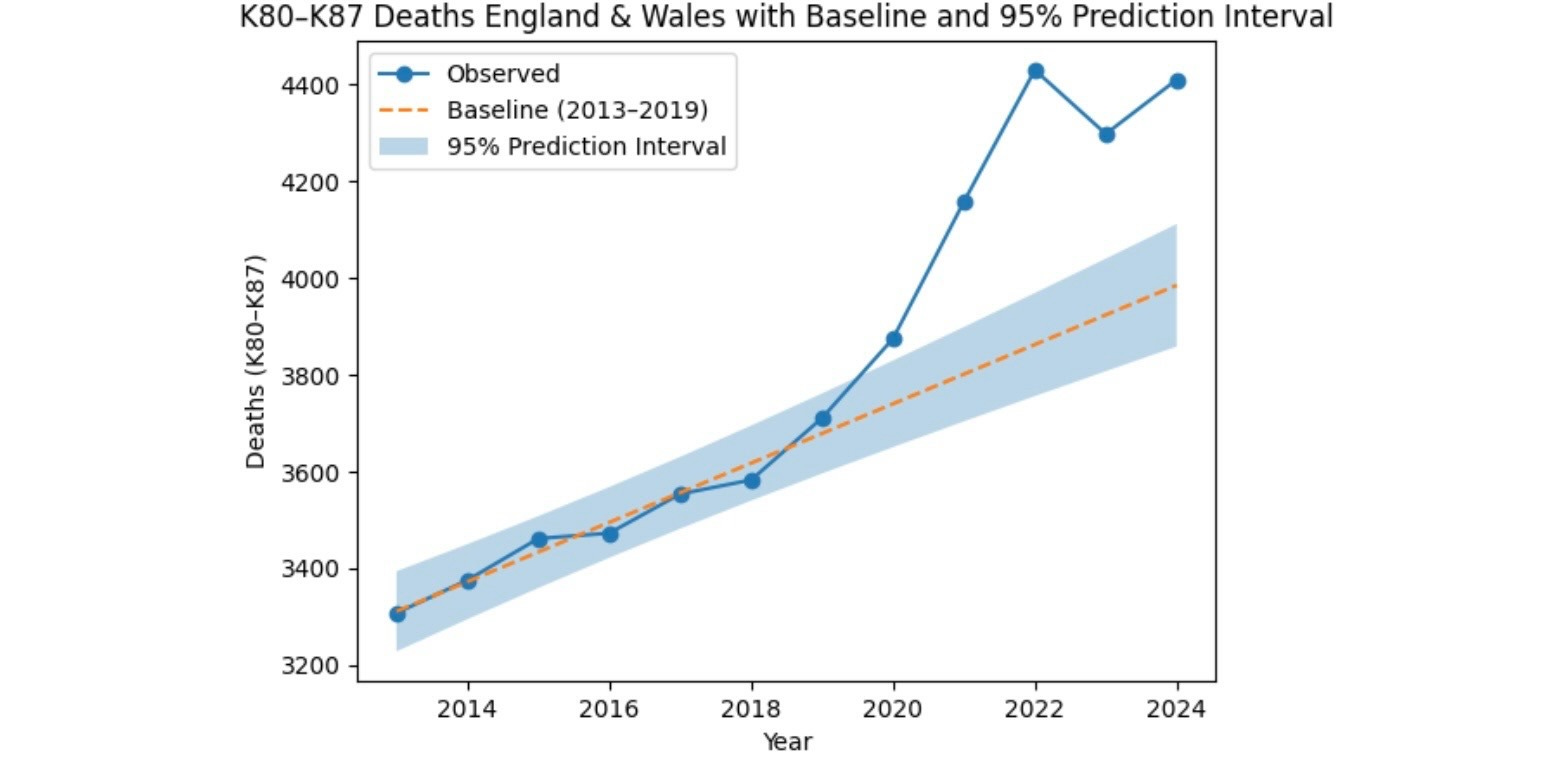
Deaths from gallbladder, biliary tract and pancreatic disease were gradually increasing, at a remarkably constant rate, before the pandemic. After a significant rise in 2020 numbers surged to peak in 2022 and have remained elevated well above the projected baseline. There were about 1,900 more deaths than expected between 2020 and 2024. Formal statistical testing suggests that the deviation from the pre-pandemic trend is unlikely to be due to chance alone, although these estimates should be interpreted cautiously given the limitations of time-series modelling using linear regression to generate an estimated baseline. Emphasis will therefore be placed on the magnitude and consistency of deviations from the baseline across multiple datasets, rather than on formal statistical significance testing.
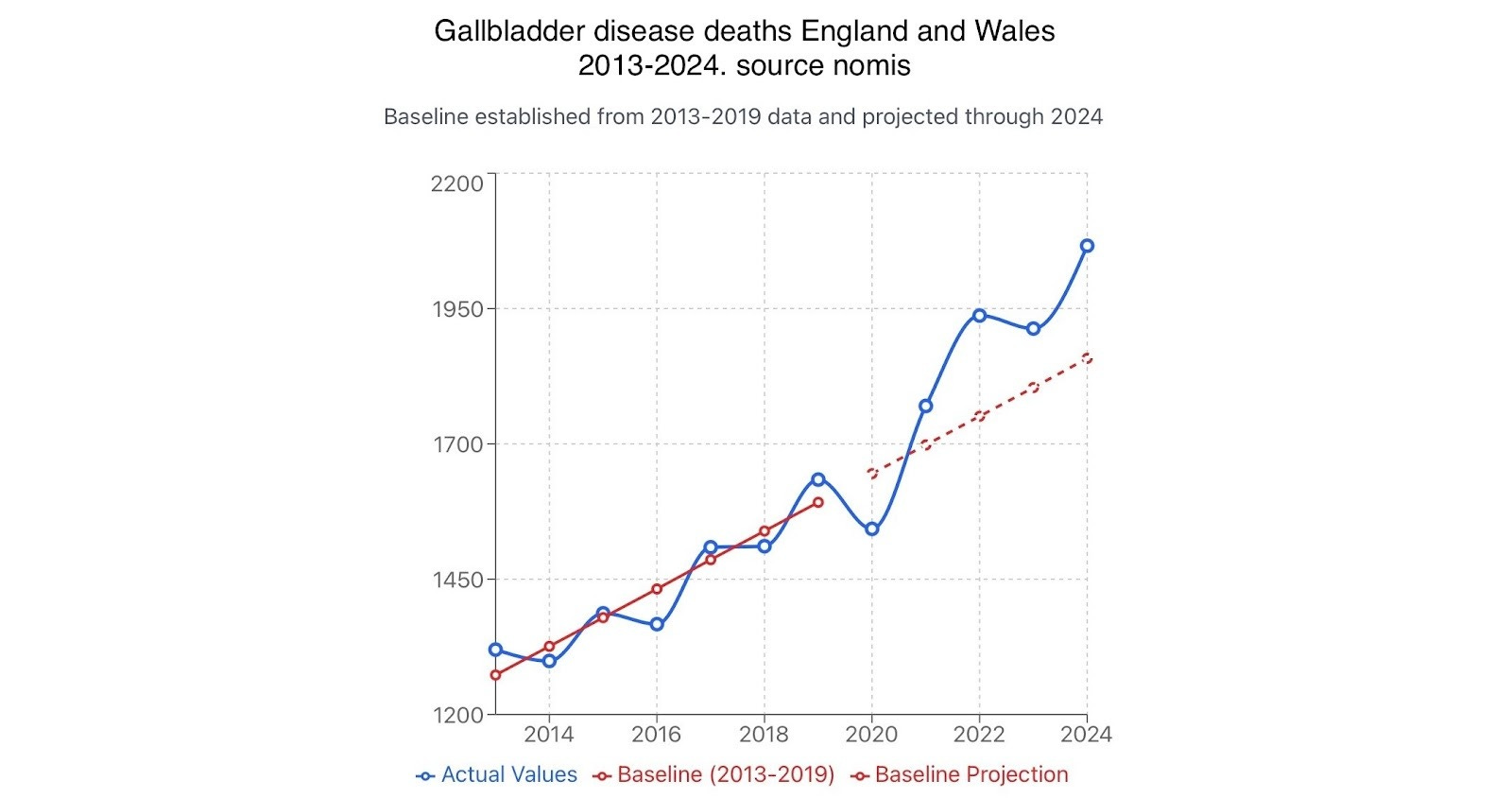
Figure 4. Cholelithiasis deaths England and Wales, ONS nomis.
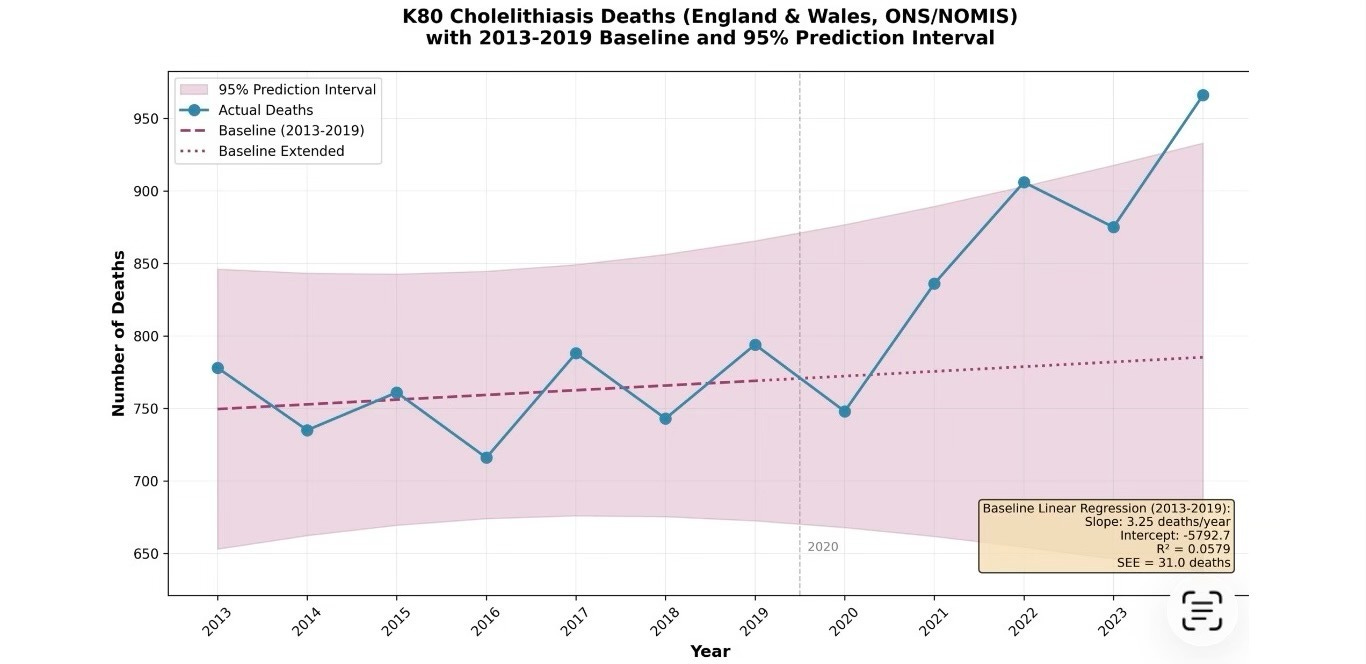
About 575 of these excess deaths were due to gallstone and gallbladder disease (K80-82) from 2021 to 2024, of which about 462 were due to gallstones, that is cholelithiasis K80, showing a clear and sustained deviation. The trend line for expected deaths 2020-2024 is based on 7 years of data (2013-2019) as ONS nomis figures start in 2013.
What contributed to the excess deaths? Seven possibilities to consider.
Demographic changes
Direct effects of SARS-CoV-2 infection
Increased alcohol consumption
Changes in surgical practice
GLP-1RA and dual action prescriptions e.g. Mounjaro and Ozempic:
Healthcare system disruption.
Covid-19 vaccination
Demographic changes: The population is aging, but this explanation is not supported by the pattern seen in figure 3 where the rate of increase in deaths is 67 deaths per year from 2013-2019 but doubles to about 134 deaths per year from 2020-2024. Also it is those in middle age that have a higher risk of developing gallbladder disease.
Direct effects of SARS-CoV-2 infection on gallstone, gallbladder and pancreatic disease: Gallstone disease has not been identified as a feature of Covid-19, however in 2020, there were a small number of case reports of associated gangrenous cholecystitis. Asti et al. reported 3 cases of acalculous (without gallstones) gangrenous cholecystitis during recovery from Covid-19 pneumonia. Bruni et al. report a 59 year old man who was admitted in acute respiratory failure on day 12 of Covid-19. He was ventilated for 8 days. During his stay in intensive care he also developed thrombosis of the femoral and jugular vein, staphylococcal septicaemia and on day 44 of his infection, gallbladder pain. The following day an ischaemic gangrenous perforated gallbladder was removed successfully. But a direct effect of infection is not supported by the publicly available nomis data which recorded a decrease in gallstone and gallbladder disease deaths in 2020 (figure 13).
Regarding Covid-19 and acute pancreatitis (AP) Babajide OI et al. concluded: ‘There is currently no evidence to point to an association, but that can be blamed on the paucity of data and also AP being infrequent in patients with COVID‐19’. Also despite ‘a myriad of complications seen in patients with COVID‐19 infection and AP such as necrotizing pancreatitis, diffuse hemorrhagic pancreatitis …. we did not find enough data to conclude that patients with COVID‐19 were more likely to have complications associated with AP as compared with patients with AP alone.’
Figure 5. Pancreatic disease deaths, ONS nomis.
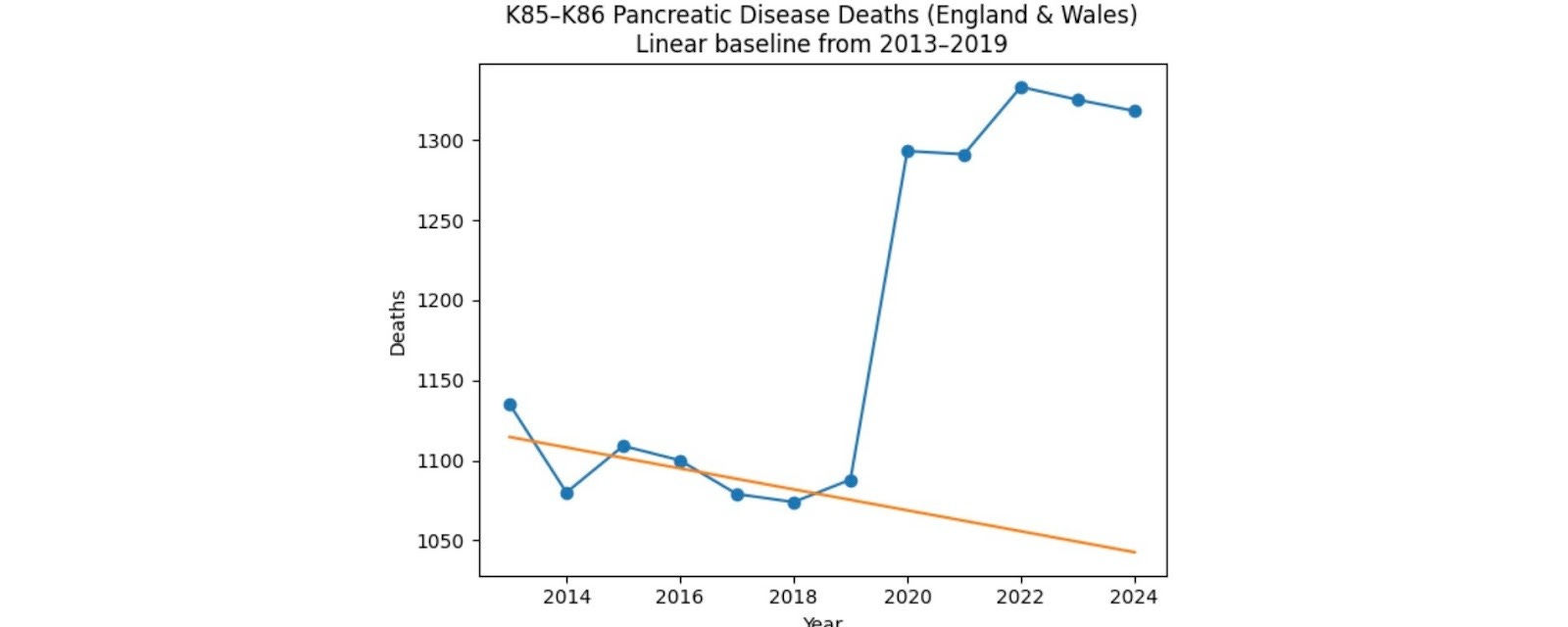
In figure 3, excess deaths in 2020 are due to a rise in pancreatic disease deaths only, including gallstone pancreatitis (figures 5 & 6). Pancreatic disease excess deaths have remained elevated by about 250 per year since 2020, instead of continuing to decline.
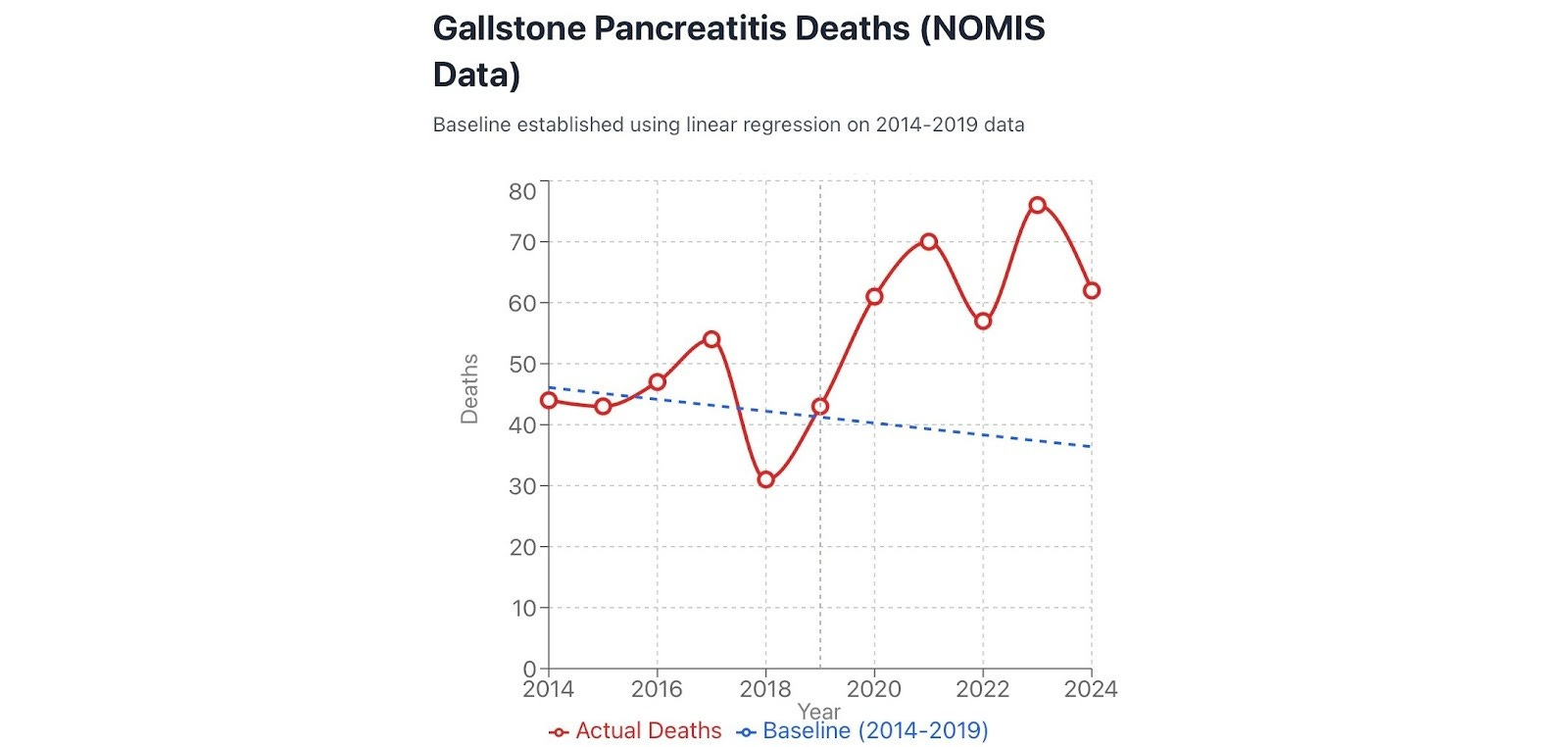
Figure 6. Gallstone pancreatitis deaths.
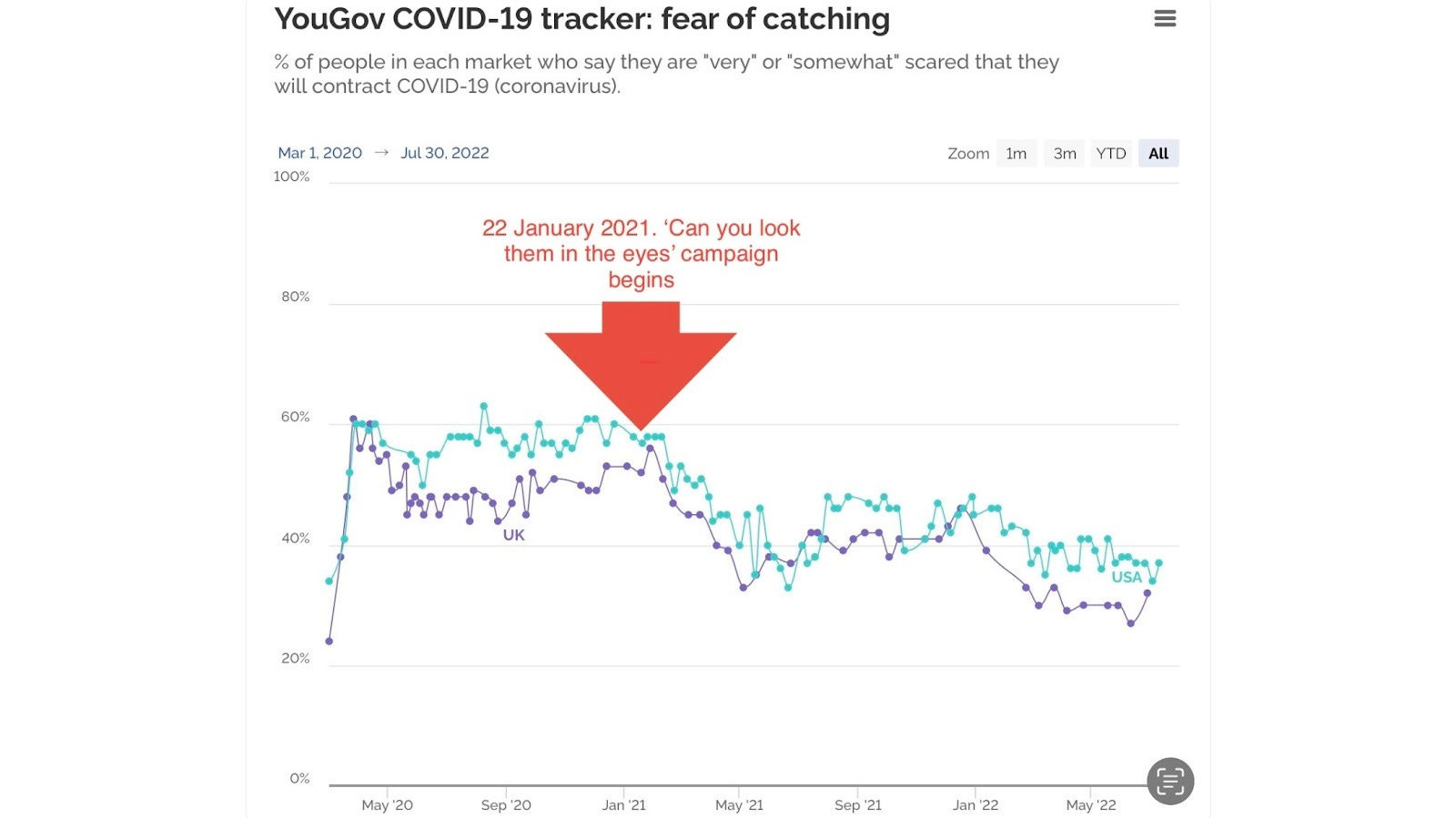
Increased alcohol consumption: The Institute of Alcohol Studies states: ‘several surveys have found between a fifth and a third of people reported drinking more during lockdown’. How much of the increased consumption during lockdowns was caused by the stress of social isolation and how much was caused by a government programme of psychological manipulation to increase guilt, shame and fear of catching, spreading and dying from Covid-19? My own fear levels were regularly tracked by YouGov. Kate Magee, of Campaign magazine, questioned whether the media campaign would ‘likely just … terrify those already following the rules’, according to Wikipedia. An intuition consistent with subsequent polling.
Figure 7. Fear tracker UK and USA - very or somewhat scared - (source YouGov with additions in red).
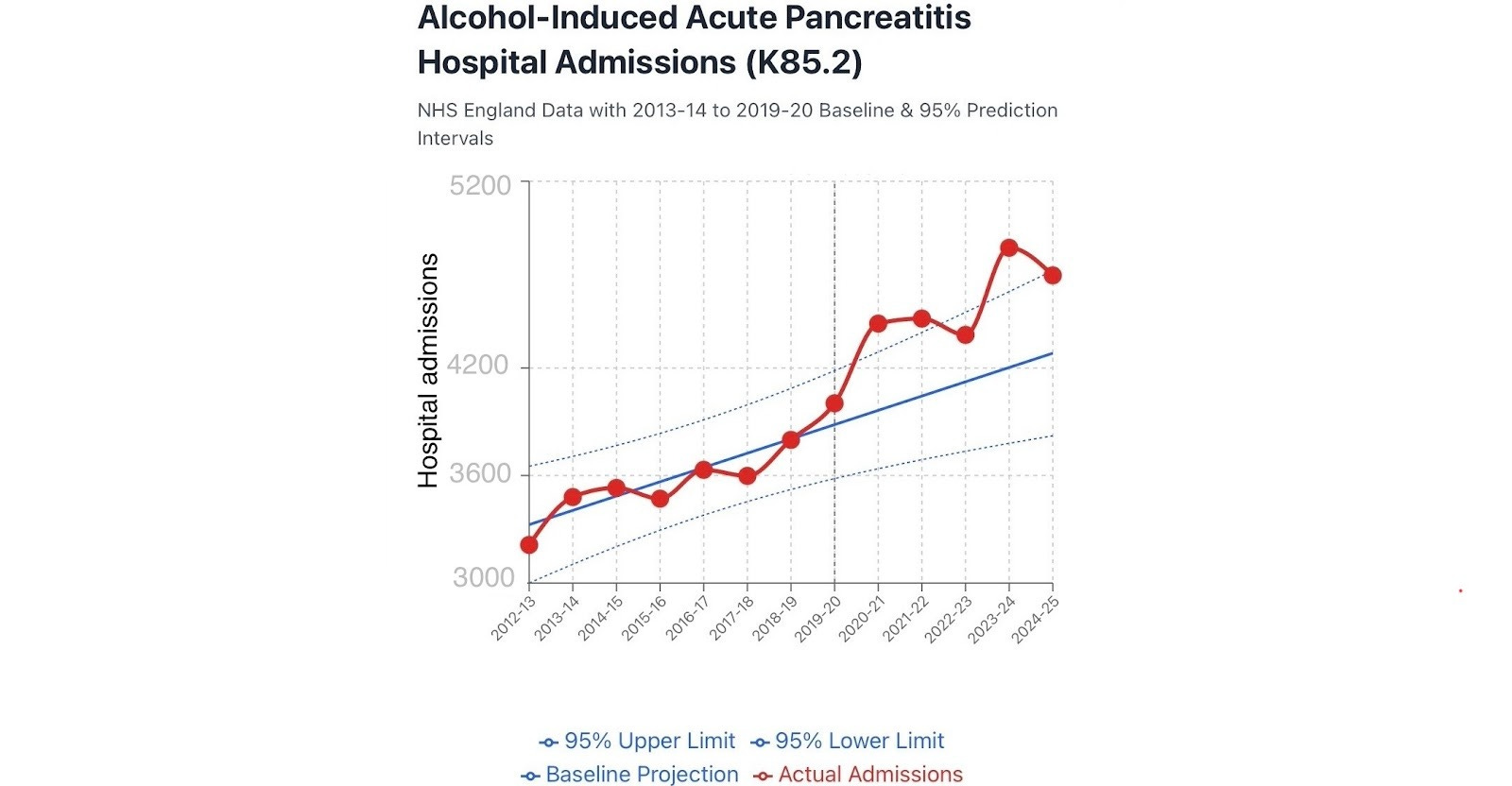
Alcohol-induced acute pancreatitis excess deaths and hospital admissions began in 2020 and peaked in 2023. There were about 2,281 admissions above the expected over the past 5 years.
Figure 8. Alcohol-induced acute pancreatitis, NHS England Digital. Hospital Admitted Patient Care Activity.
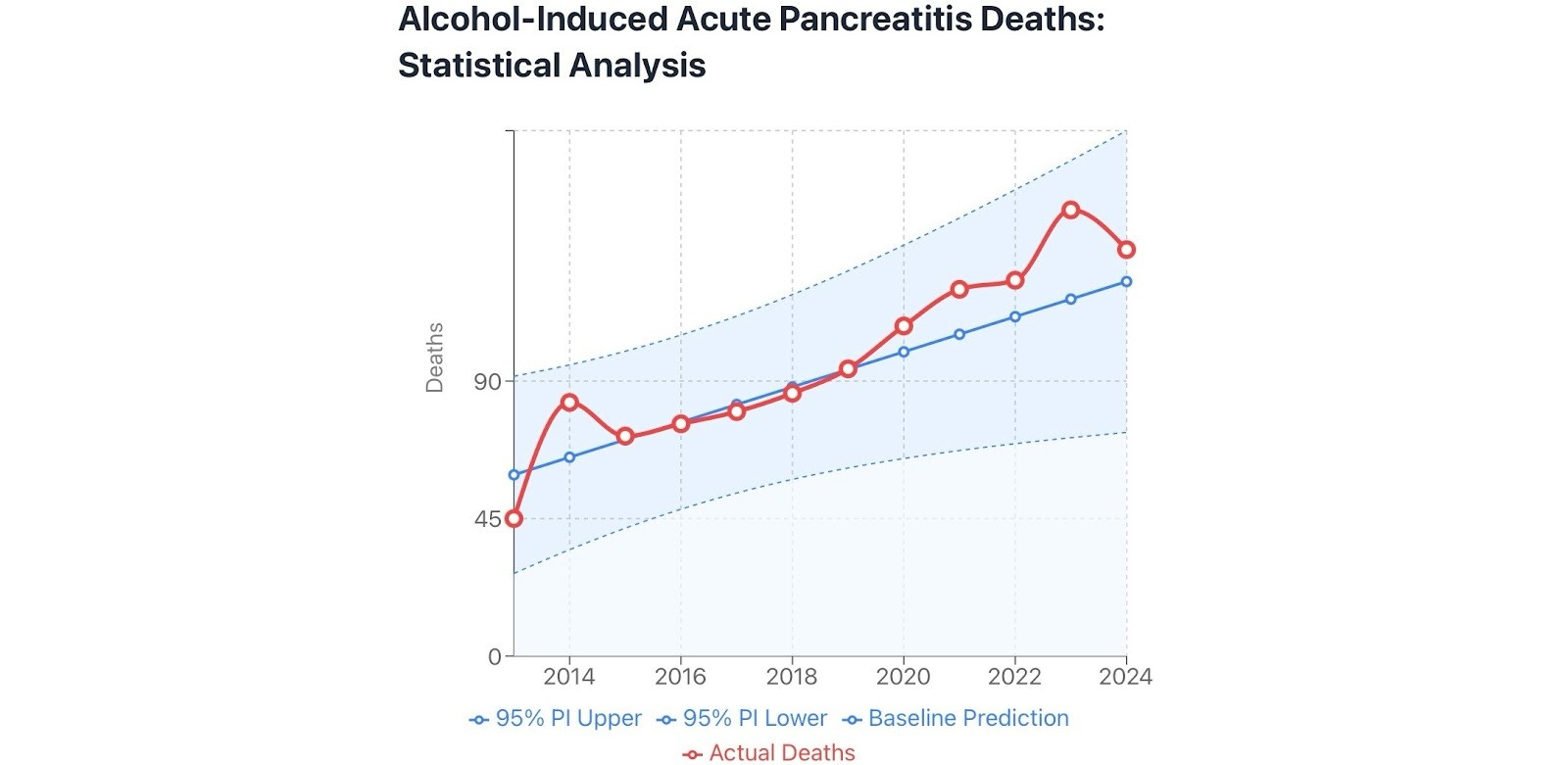
There were about 74 excess deaths due to alcohol-induced acute pancreatitis 2020-2024.
Figure 9. England and Wales. Source ONS nomis.
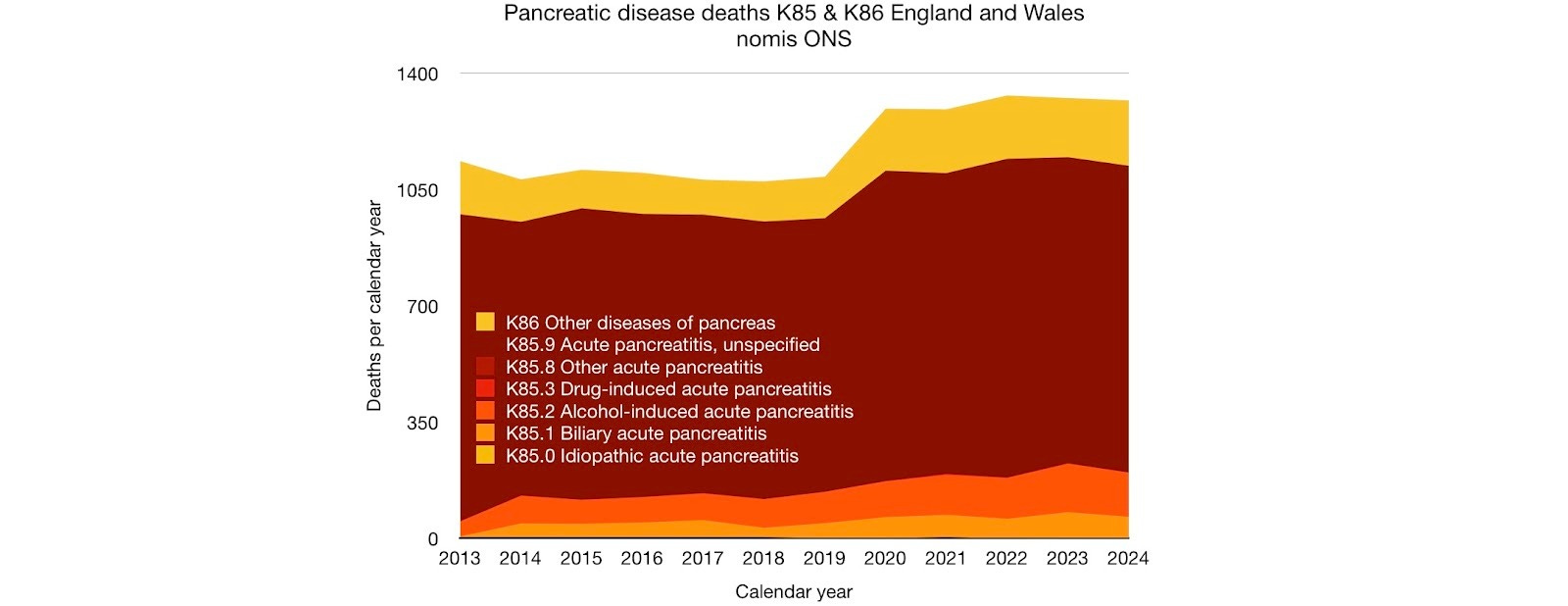
More detailed analysis of the public data on deaths due to pancreatic disease is hampered because most deaths are classified as acute pancreatitis unspecified. The proportion of these deaths caused by: alcohol consumption (lockdown stress and fear); late presentation or gallstone complications (disruption to services); Covid-19 infection or vaccination, remain unknown.
Figure 10. Most pancreatic disease deaths are coded as acute pancreatitis unspecified.
Changes in surgical practice suggested, included: in those testing positive for Covid-19, ‘to postpone surgical treatment until the patient is no longer considered potentially infectious or at risk of perioperative complications’ and that ‘surgical theatres were converted into additional ICUs’. General guidance for surgeons working during the pandemic was issued in March 2020 on how to prioritise emergency surgery. Another report on cholecystitis treatment states that ‘sites stopped laparoscopic surgery and managed patients conservatively using drains or antibiotics’. Further guidance on restarting elective surgery was issued in May 2020. This explanation is not supported by the nomis data (figure 13) as there was no rise in gallstone and gallbladder deaths in 2020, instead there was a 6% or about 102 death deficit from the expected number.
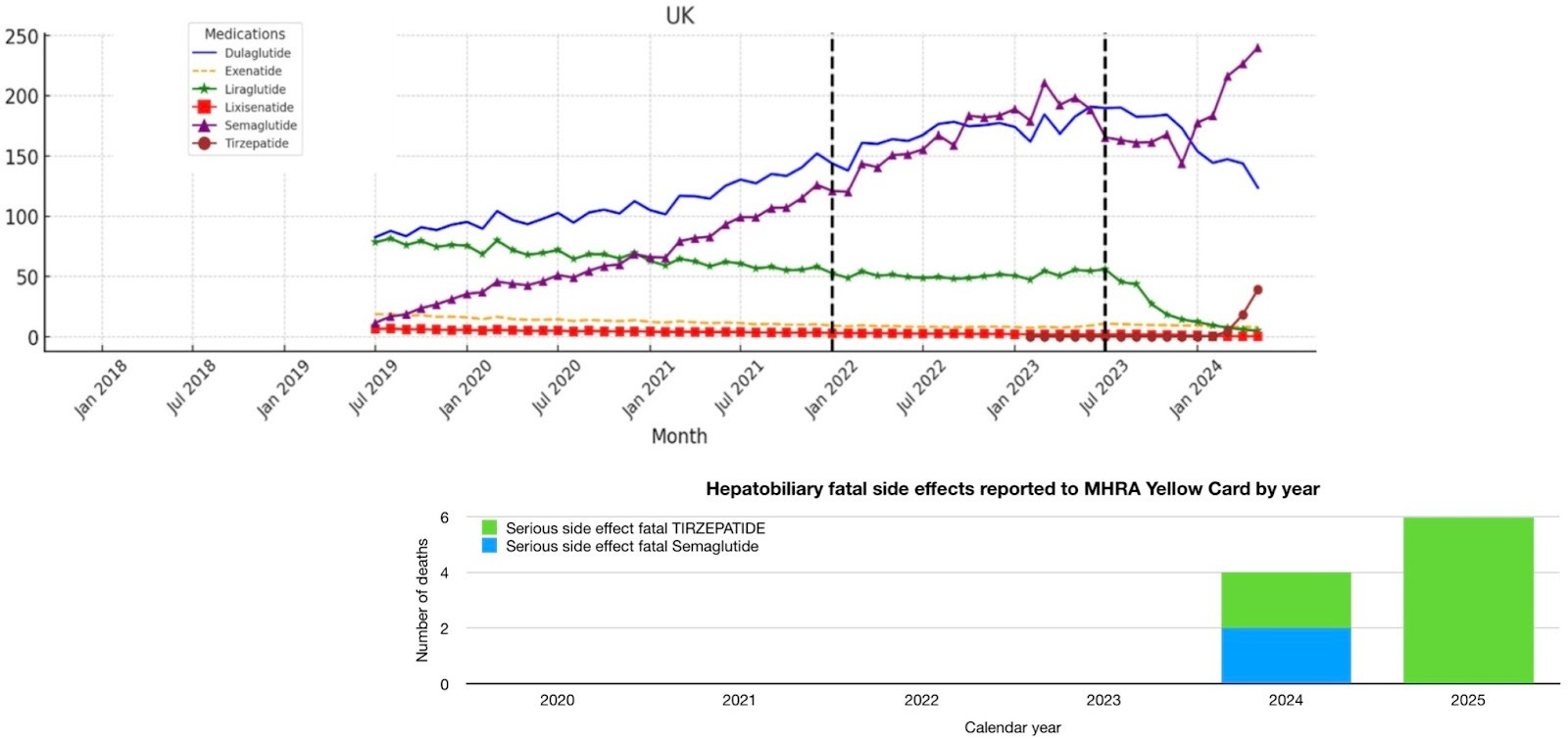
Semaglutide prescribing rose steadily from 2019 (figure 11). The MHRA has updated its guidance for GLP-1 prescribers and patients regarding the risk of severe acute pancreatitis in patients taking GLP-1s. Also Ramírez-Mejía et al. concluded: ‘Current clinical evidence suggests an increased incidence of gallbladder-related adverse events with GLP-1RAs treatment, particularly at higher doses and for longer periods’. Prescriptions increased at about the same rate from early 2019 to mid 2023 when there was a temporary shortage. Semaglutide was recommended by NICE for NHS use for weight loss in March 2023 and launched in England for weight reduction in September 2023 when supplies became available. An inflection point can be seen at that time, in the graph below, when prescribing of Semaglutide increases and prescribing of Tirzepatide (Mounjaro) for weight loss begins. The MHRAs Yellow Card website reports 2 deaths due to hepatobiliary disease following Semaglutide, both of which were in 2024, and for Tirzepatide 2 deaths in 2024 and 6 in 2025 (figure 11). None were reported before these dates. This is a potential contributor to the excess gallbladder disease deaths from 2021 onwards, but with the contribution likely small initially and increasing from 2024 as weight-loss prescribing accelerated. Time may make the size of the contribution clearer. GLP-1RAs were already being prescribed for type 2 diabetes before 2019 and any effect on gallbladder disease deaths from those prescriptions will be included in the 2013-2019 baseline calculation. The MHRA Yellow Card website uses MedRA to classify side effects so pancreatitis deaths are classified with gastrointestinal rather than hepatobiliary disorders (unlike in ICD-10).
Figure 11. GLP-1 Receptor Agonist prescriptions per 100,000 population UK from Impact of ADA Guidelines and Medication Shortage on GLP-1 Receptor Agonists Prescribing with MHRA Yellow Card hepatobiliary disease fatality reports below.
Healthcare system disruption 1 - missing cholecystitis admissions.
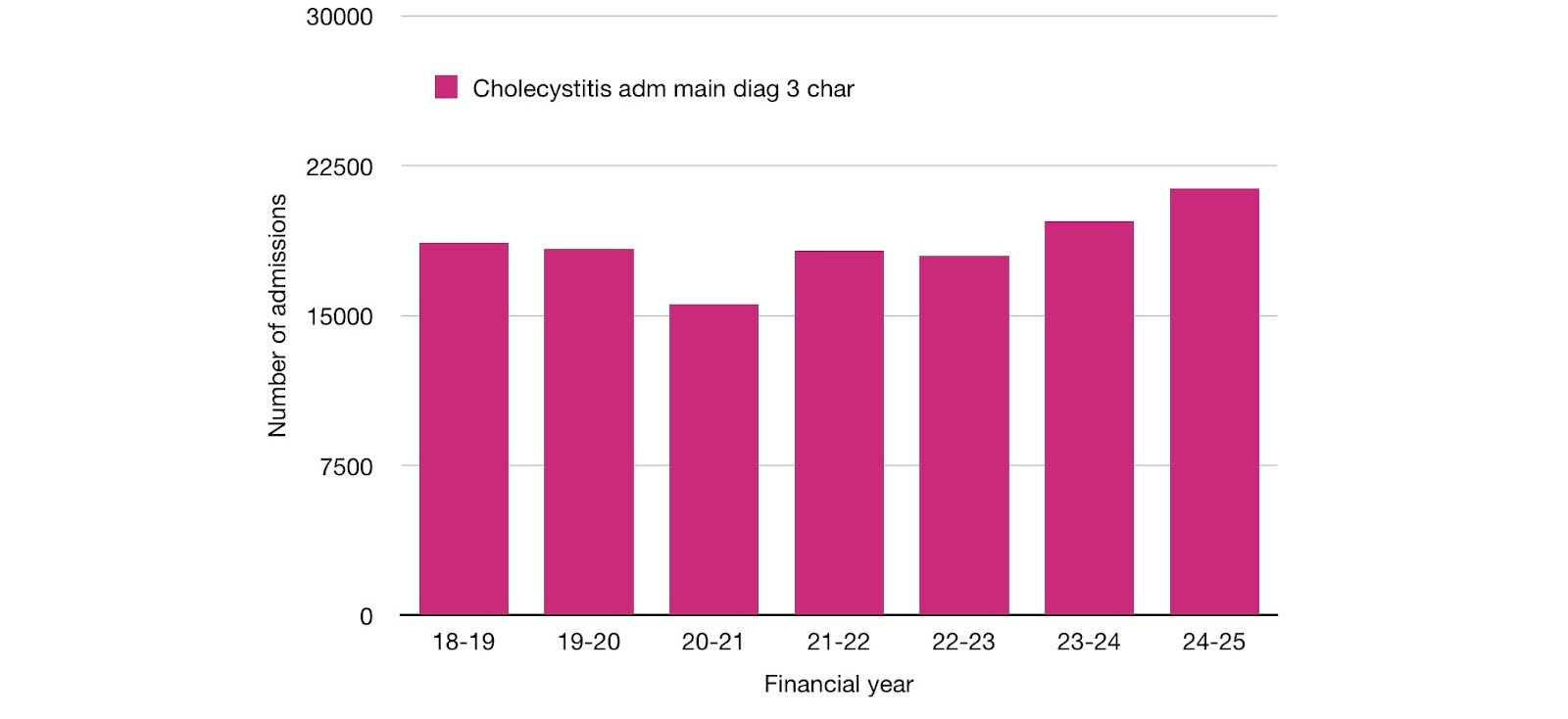
That there was disruption can be seen in the 2,765 or 15% drop in hospital admission numbers for cholecystitis as a main diagnosis. In England, admissions dropped from 18,343 in 2019-2020 to 15,578 in 2020-2021. Cholecystitis sufferers were more likely to stay at home during an acute attack in 2020-2021, possibly protecting the NHS or too afraid to go to hospital for fear of catching and dying from Covid-19.
Figure 12. Cholecystitis K81, hospital admissions, Hospital Episode Statistics (HES) Hospital Admitted Patient Care Activity, primary diagnosis 3 character, England.
Despite this, there was a decrease in gallstone and gallbladder deaths during the period of maximum disruption in 2020. On the surface, this drop in deaths in 2020 suggests that: even if patients with cholecystitis avoided or delayed going into hospital because of the disruption, their condition did not become more likely to be severe, untreatable and fatal.
Figure 13. K80-82 gallstone and gallbladder disease deaths.
However this scenario of delayed presentation and advanced disease in 2020 could still have happened and been masked in the data, if the disruption was so profound, as is suggested in the guidance below, that patients died at home, alone, having been denied social contact, undiagnosed due to restricted healthcare and without the post-mortem they would normally have had, their deaths attributed to other causes. As most would have had a fever and many would have kept paracetamol in the house, death could even have been misattributed to Covid-19. The lack of rigour required to attribute cause of death to Covid-19 is alarming and likely contributed significantly to making the first wave of Covid-19 deaths larger. The guidance on death certification given to doctors in Scotland on 20th May 2020 stated:
‘2. There may be cases where there has been little or no recent medical intervention and the medical practitioner is short of information as to the deceased’s recent state of health. In these circumstances, the medical practitioner should consider the symptoms outlined above from relatives or friends, if available, as well as looking at the wider facts and circumstances. These wider facts and circumstances can include the fact that there is a COVID-19 Pandemic, that the COVID-19 Pandemic has struck in the locality, whether there was any evidence of medication suitable for treating the symptoms of a COVID-19 Pandemic found in or near the deceased’s possessions e.g. analgesics, cough medicine, medicines to reduce the fever, etc.
3. There may also be cases where the medical practitioner finds some evidence of symptoms and/or surrounding circumstances that are compatible with, but perhaps not exclusive to, COVID-19 disease as being the cause of death. In such a case, and where there are no other indications as to the cause of death, and where there are no suspicious circumstances, it would be considered clinically responsible to certify the death as “presumed COVID-19 disease”. This will be accepted as a cause of death by the local authority registrar and recorded in that format in the register.’
This CHOLECOVID study paper compares severity of cholecystitis hospital cases admitted during the first 8 weeks of the pandemic (4,278 admissions March-May 2020) with a similar 8 week prior period (5,505 admissions September to November 2019), in a global sample, and found a small but statistically significant (p-value <0.001) increase in the proportion of Tokyo severity grade II moderate (30% increased to 35%) and severe (3.8 increased to 4.1%) cases. Thirty day mortality based on 13 deaths in each group was 0.4% prepandemic and 0.6% in the first 2 months of the pandemic (p-value 0.355).
Healthcare system disruption 2 - missing cholecystectomy operations.
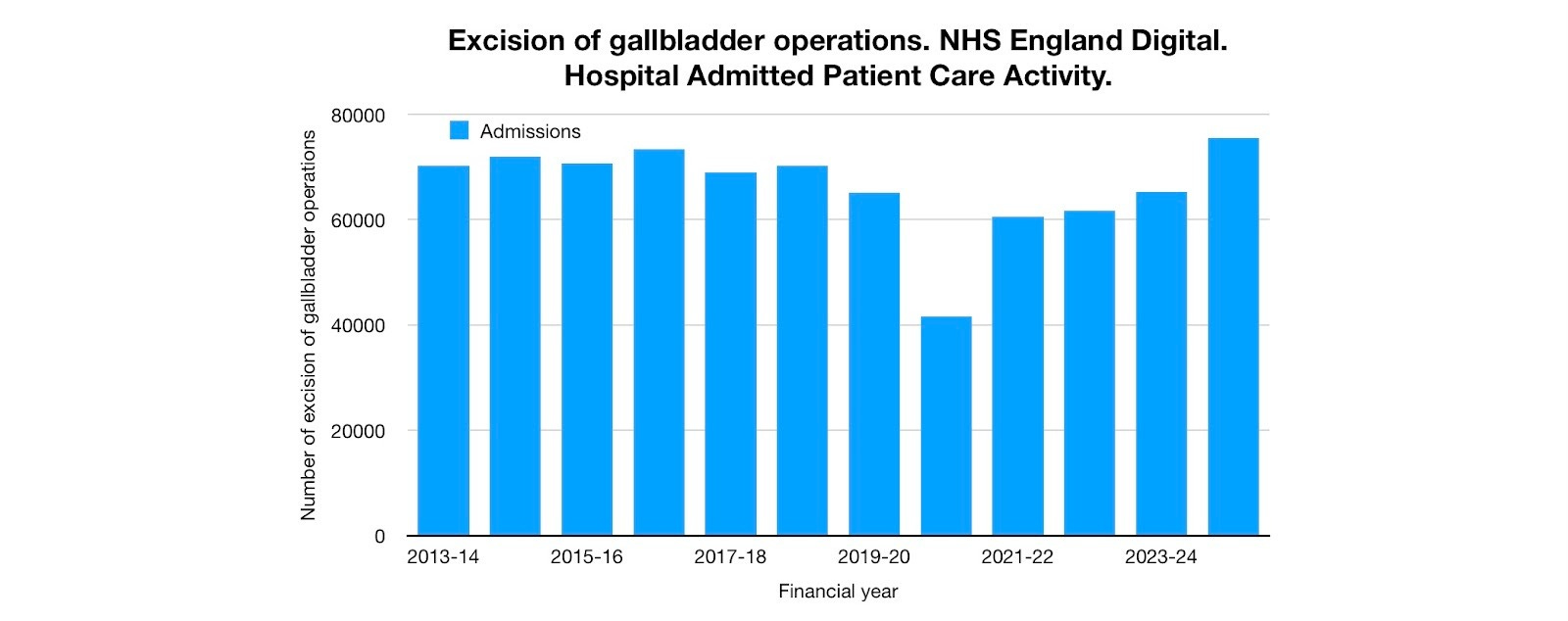
Even greater disruption can be seen in the reduced number of cholecystectomy (excision of gallbladder) operations to remove both gallstones and the gallbladder. 23,491 (36%) fewer operations were done in the first year of the pandemic than in the year before. Only about 12% of this drop can be accounted for by the drop in acute cholecystitis admissions.
Figure 14. Cholecystectomy operations J18 HES/HAPCA procedures and interventions primary procedure 3 character.
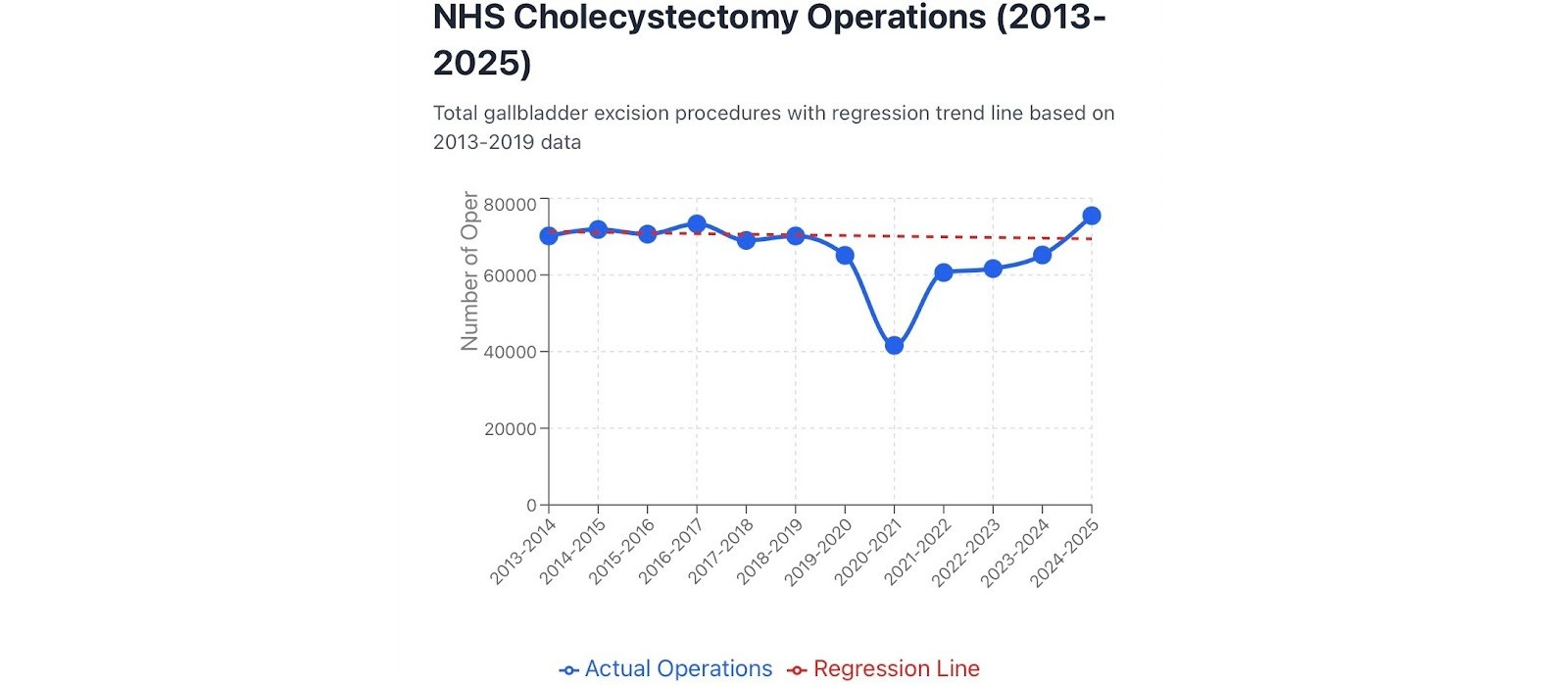
Linear regression gives an estimate of the total reduction in number of operations over 5 financial years (April 2019-March 2024) of about 55,479. That represents the equivalent of almost an entire year (about 80%) of operations.
Figure 15. Cholecystectomy operations with pre-pandemic baseline.
NHS Digital Hospital Episode Statistics or Hospital Admitted Patient Care Activity statistics already include NHS commissioned activity in the independent sector, but some of these missing NHS operations may have been privately funded in the independent sector instead. The numbers are not available. However the Nuffield Trust states that while the total number of procedures done in the NHS dropped from 9.8 million in the year before the pandemic to 6.6 million in the first year of the pandemic, the number of procedures done in the private sector also dropped by about a third from 1.2 million to 0.8 million. It is therefore unlikely that many of the missing NHS operations were privately funded.
Healthcare system disruption 3 - missing procedures
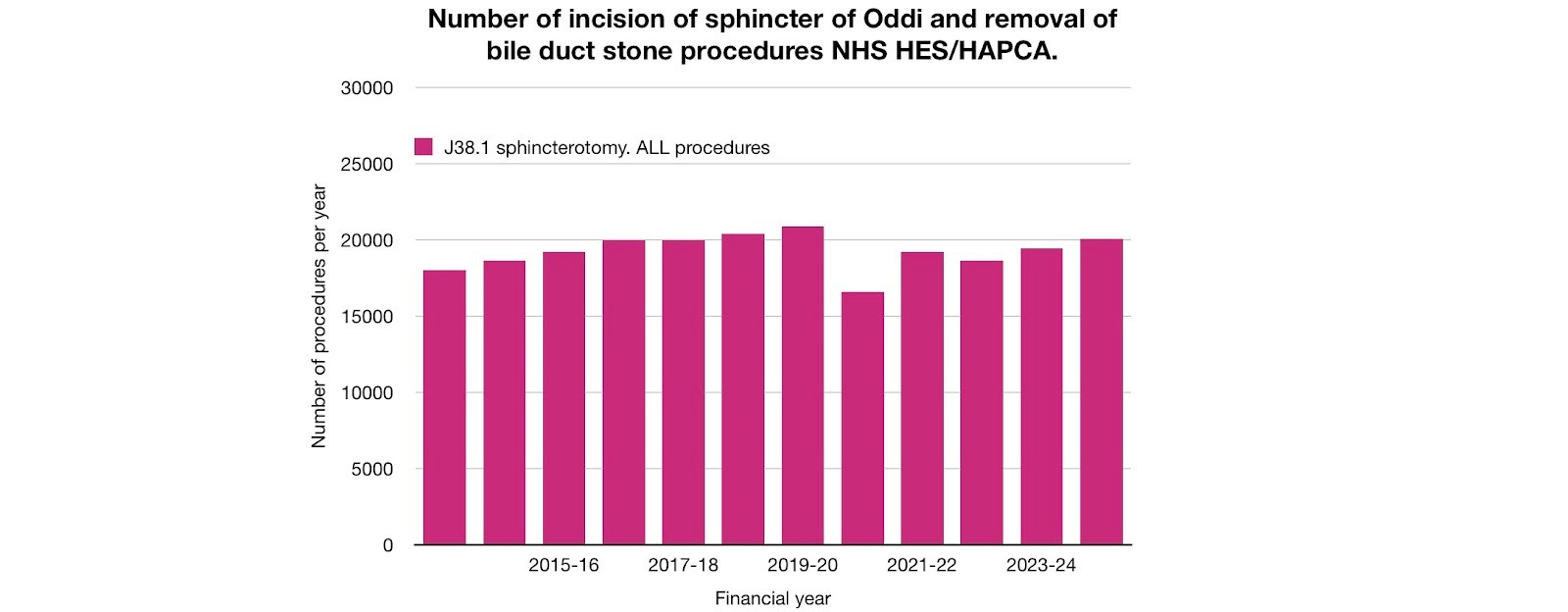
For the approximately 1 out of 4 bile duct stones that do not pass spontaneously, endoscopic incision of the sphincter of Oddi can be used to enlarge the opening of the bile duct into the intestine, as explained in a) a 1 minute animation, b) in 4 minutes by a Mayo Clinic doctor and c) in a 3 minute video of a case study as seen through an endoscope.
In the year before the pandemic 20,870 endoscopic incision of sphincter of Oddi and removal of stone procedures were done in England. In the financial year 2020-2021 this figure dropped by 4,308 (21%) to 16,562. The number has not yet fully recovered.
Figure 16. Missing endoscopic procedures to remove bile duct stones (NHS HAPCA all procedures, 4 character).
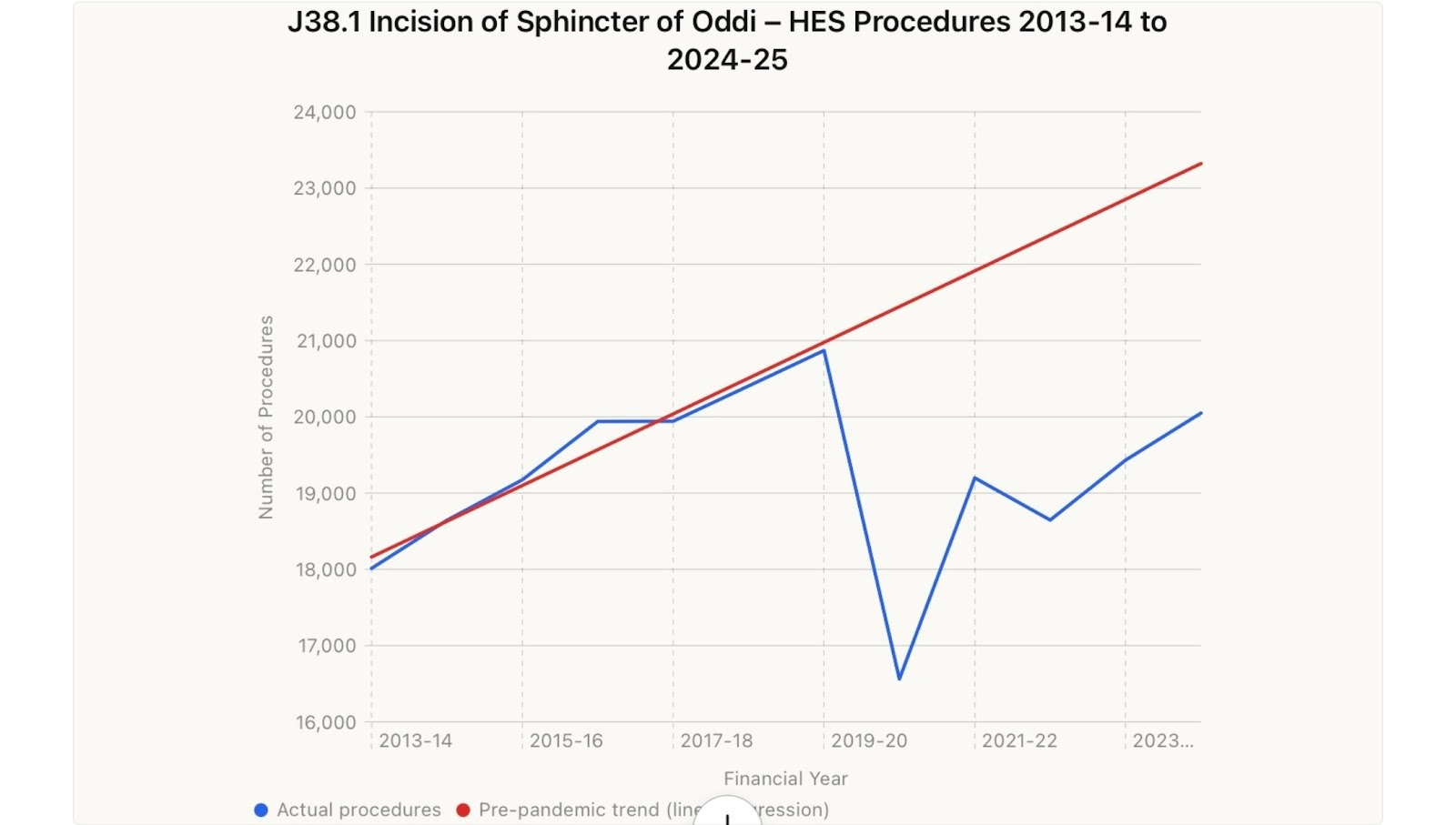
Linear regression estimates the cumulative deficit over 5 years to be about 18,027 procedures, the equivalent of almost an entire year of procedures. Even in the year 2024-25 the deficit was about 3,272 procedures and still below pre-pandemic levels.
Figure 17. Missing endoscopic procedures to remove bile duct stones (NHS HAPCA all procedures, 4 character) linear regression.
Conclusion
About 1,900 excess deaths from gallbladder, biliary tract and pancreatic disease were associated with approximately 55,479 missing cholecystectomy operations, 18,027 missing endoscopic bile duct procedures, and 2,765 missing NHS hospital admissions for acute cholecystitis. Some of the excess pancreatic disease deaths were associated with alcohol consumption, with the increase likely due to lockdown isolation-stress and fear. There is also a possibility that pancreatitis deaths were increased by Covid-19 infection. But neither of these reasons can account for the approximately 575 excess deaths from predominantly gallstone-related gallbladder disease since 2021. GLP-1RAs were being increasingly prescribed over this period but at present, any effect on excess gallbladder disease deaths appears to have been small before 2025. In the absence of another explanation, most of the pre 2025 excess deaths discussed here are likely due to disruption to healthcare services. The 575 excess K80-82 deaths are spread over 4 years with an average 8% increase over the projected baseline, but reaching about 11.2% in 2024.
Although gallbladder disease deaths only represent a small percentage of the approximately 577,000 deaths per year in England and Wales over the past 4 years, they are likely to reflect the level of harm caused by service disruption across other areas of medicine and surgery. The Nuffield Trust figures suggest 3.2 million fewer procedures were done in the NHS in the first year of the pandemic. How many of these also led to deaths that were preventable deaths in normal circumstances? Deaths due to healthcare disruption should be an important consideration of the Covid Inquiry. In module 3, the Inquiry only considered 4 examples: colorectal cancer, ischaemic heart disease, hip replacement surgery and inpatient mental health services for children and young people. These findings suggest that the indirect harms identified by the Inquiry, may be broader and more prolonged, than currently appreciated.
On the 6th anniversary of the first lockdown, where has what started as - 3 weeks to ‘squash the sombrero’ - left us? Over 40,000 cholecystectomy operations are still missing, although there are signs of the start of a catch-up in 2024-25. Endoscopic removal of bile duct stone procedures are still about 3,000 procedures per year below the projected prepandemic baseline. Meanwhile, K80 cholelithiasis or gallstone disease deaths show not only sustained, but worsening excess mortality, with the latest figures reporting deaths in 2024 elevated about 23% above baseline projections.
In the next part I will look at these excess gallbladder deaths in more detail before moving on to consider if there is a possibility that Covid-19 vaccines may have also contributed to excess gallbladder deaths.
What a wonderful article..!
If only certain other medical practitioners were so assiduous..!
This is a fantastic piece of research, thank you. I am so saddened to read this. I can only begin to imagine the full weight of COVID policies on the impacted individuals.
My mother nursed my father at home, he had dementia, when drugs were withdrawn a week before his death, she was left without any visit from a medical professional, they would not even attend to drain the white fluid that was building up in his throat. Instead they directed us to source equipment that we could not find and left his family to try to clear the liquid themselves. I remember receiving a call from a nurse the on the day he had died asking if she should come out. It was all too late.
I hope this is shared far and wide and I especially hope that it is forwarded to to those who did not heed or outright dismissed our warnings back in 2020.