


Why did the minister reference Singapore?
Claims of higher cardiac deaths in the unvaccinated


On Friday 20th October, at the debate on excess deaths, Maria Caulfield, the Parliamentary Under-Secretary of State for Mental Health and Women's Health Strategy said,
“A recent study in Singapore actually found that when they looked at patients who recovered from covid who were unvaccinated, they showed an increased risk of, like, 56% more to be at risk of cardiac complications a year later compared to those who were vaccinated. So there is conflicting data on this and I'm not necessarily disagreeing with him, but I think we need to have a robust conversation on this and not to assume that one side necessarily has all the answers.”
While we commend her willingness to have a further debate on this topic, it is very telling that having been presented with copious UK data, she had to fall back on a single study from Singapore. Let’s take a closer look at that Singapore paper.
The paper Maria Caulfield references was a study that ran for three months from September to November 2021. It seems reasonable to pick the Delta wave for this study which ran from September to the end of December. But why omit December? What is even more odd is that the control group, those who tested negative, recruited from April 2020 to December 2022 - for 33 months! There were surely plenty more people testing negative than positive so why were the positive test results from such a short time period?
Including the vaccinated as “unvaccinated”
In the study they critically fail to define “unvaccinated”. However, a clue comes from the fact that the sum of the “unvaccinated,” and those with two doses or three doses equals every one who tested positive (see figure 1). This presumably means that everyone who had been vaccinated but had not yet been “fully vaccinated” were described as “unvaccinated”.
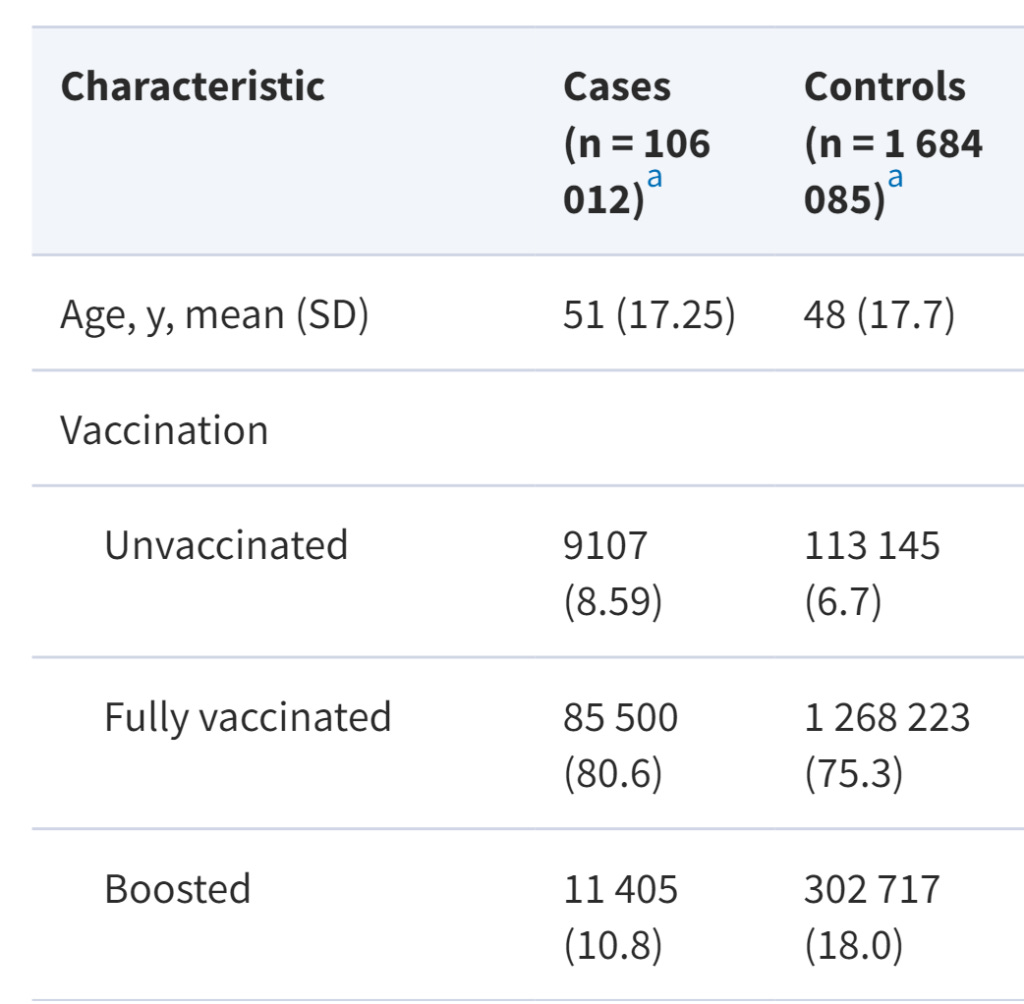
Of those who tested positive 91.5% were “fully vaccinated” or more. Given that at the end of the study only 85% of the population were in this group, even with the most generous interpretation the risk of testing positive was clearly higher in those who had been vaccinated (see table 1).
During this time the number vaccinated rose from 4.59 million to 4.82 million - meaning the unvaccinated were 3.6% to 8.2% of the eligible population. (In 2021, the population was 5,454,000 only 5 million of whom were over the age of 12 and eligible for vaccination. The study excluded under 18 year olds). Therefore between 55 and 58% of the “unvaccinated” in the study were actually vaccinated and if they classified those within two weeks of the second dose the proportion would be even higher.
Covid is not the cause of commonest heart problems
Testing was compulsory when interacting with the healthcare system. Patients in hospital would be exposed to high levels of virus in the air so would be at increased risk of testing positive. It is therefore no surprise to find these people are sicker than those testing negative.
The paper concludes that there was no significant association between covid and any specific type of thrombosis, ischaemic heart disease, acute coronary disease, myocardial infarction, ischaemic cardiomyopathy or angina. The minister therefore shared a study which confirms Andrew Bridgen’s (and HART’s) conclusions about Australia proving that covid is not the cause of the increase in heart problems. However, when combining all these problems they did see a slightly higher risk for any problem among those testing positive. They did also make the claim that unvaccinated survivors of covid had higher rates of ischaemic heart disease, rhthym and other disoders.
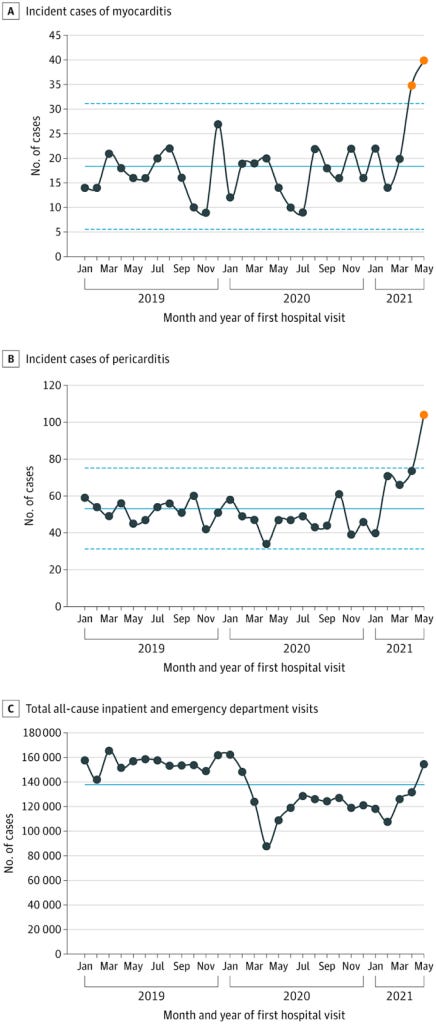
They say, “COVID-19 survivors did not exhibit higher risk of all inflammatory heart disease” indicating that covid was not linked to myocarditis and pericarditis. However, they also claimed an increased risk of heart failure and non-ischaemic cardiomyopathy (which would include post myocarditis problems) in those post covid.
Maria Caulfield used this paper to allege a higher rate of post covid heart conditions among the “unvaccinated”. Remembering that half of the “unvaccinated” in this study were in fact vaccinated, what does that mean?
Cardiac and other risks in early post vaccination period
It is well established that the risk of hospitalisation from covid in the period immediately after vaccination is well above baseline levels and this is likely to be because of the known period of immunosuppression that follows vaccination. Furthermore this period includes a higher rate of infection than in the unvaccinated. It is quite disingenuous to compare people in this period as if they were “unvaccinated”. This group would also have a significant risk of having vaccine induced heart injury and it is ludicrous to include such a group in an assessment of post covid heart problems among the unvaccinated.
Almost all studies looking at the incidence of myocarditis overall shows the rise only began after vaccination. Therefore any association of post myocarditis effects after covid will have been in the vaccinated population, even if in this paper they have been labelled as “unvaccinated”.
Big picture on heart complications in Singapore
To fully understand the study, it is important to look at the big picture.
There has been a huge increase in cardiac deaths in Singapore. Can these really be attributed to only the tiny unvaccinated population, most of whom are children?
Singapore makes for an interesting case study as they were vaccinated before having any significant covid deaths. There were only 29 covid attributed deaths prior to September 2021 and 799 in all of 2021. A thorough analysis of data since 2000 shows that there were 1534 excess circulatory deaths in 2021.

Monthly mortality data shows a clear rise in the gradient of non-covid deaths after the vaccine rollout, with only a small fraction of the increase attributable to covid (see figure 4).

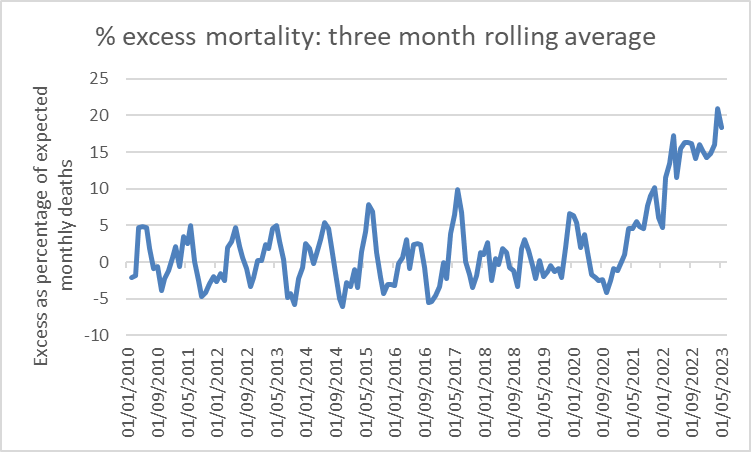
Another way to look at this data is to see the cumulative excess over and above the trend. This should fluctuate up and down around zero (see figure 3). Overall 2020 had more deaths than expected. This may in part have been due to an ageing population. However, from March 2021 there is a sharp uptick in cumulative mortality. Arguably the gradient of the rise increases further from 2022 but the total increase is far beyond what has been attributed to covid – 6521 excess deaths with only 1872 attributed to covid. (This is lower than the ballpark of 7142 for 2021 and 2022 estimated using annual data since 2000 as the baseline).

Although Singapore has produced conflicting data on death by cause, the majority of it shows there were between 600 and 1534 excess circulatory deaths in 2021.
Singapore is one of the most vaccinated nations with one of the lowest rates of vaccine hesitancy and an overall vaccination rate of 91.5%. Almost all those at significant risk of dying were vaccinated. Can excess mortality 15-20% above expected levels really be because of a problem seen only in the 8.5% of the population who are unvaccinated? If that were the case the mortality rate in that fraction of the population would have to be dying at about three times the expected average rate for the population. This would be a risk far, far higher than any increased risk claimed in the paper.
Given the high rates of cardiac deaths in Singapore, the high vaccination rates and that this paper clearly shows that covid did not predispose to such deaths, it actually supports the argument that the rise in cardiac deaths is a result, not of covid, but of the covid vaccinations.
The definition around vaccinated and unvaccinated appears to be a ploy multiple countries have used. If you died after the first vaccine, and before the two week period you died from COVID not the vaccine. If you can get your hands on the Australian senate enquiry the TGA had reduced 1,000 death certificates that said it was caused by the vaccine to just 14. They couldn’t explain how they did that.
Great take down of the "Singapore" defence