


Covid Inquiry Module 4 revisited
A Confirmed Whitewash

4 February 2025, 2⎼5pm: Church House, Dean’s Yard, Westminster, London SW1P
This detailed review is from Dr Lisa Hutchinson, who attended the meeting.
It was appallingly apparent from the very first day of the much anticipated Module 4 of the UK Covid Inquiry, that this never intended on being an honest, open examination into what happened during the pandemic to ensure the harms endured by reckless public health policies could never again be repeated. The Covid Inquiry included vaccine-injured and bereaved groups as well as officials responsible for the jab rollout. Instead, the Inquiry was a stark reminder of a whitewash intent on burying evidence challenging the official narrative that “vaccines are safe and effective”. Further still, it has continued to gaslight those who have been severely injured and harmed by the vaccines. The date for the inquiry was delayed from mid-2024 to January 2025, and the inquiry length truncated from 5 weeks to 3 weeks. A group of experts were called to submit witness statements and since transparency has been non-existent throughout the pandemic, they felt it was in the public’s interest to provide access to their expert testimonies. Thus, the experts formed The People’s Vaccine Inquiry (PVI) to make their evidence available to the public. To ensure the truth of the Covid Inquiry and people's voices could be heard, The PVI convened a press conference on 4 February 2025. This lay bare the tragic Shakespearian theatre of the UK Covid Inquiry Module 4 public hearings, which were held on 14⎼31 January 2025.
The following speakers presented at the PVI Press Conference:
Caroline Pover (Chair of Trustees) and Dr Christian Buckland (Psychology adviser), representing the UK CV Family for covid vaccine injured and bereaved
Dr Jonathan Engler and Dr Clare Craig, co-chairs of the Health Advisory & Recovery Team (HART)
Dr Elizabeth Evans, CEO representing the UK Medical Freedom Alliance
Dr Ros Jones, representing the Childrens’ Covid Vaccines Advisory Council (CCVAC)
Nick Hunt, former Senior Civil Servant in the Ministry of Defence, for the Perseus Group
Professor Angus Dalgleish, Emeritus Professor of Oncology, University of London
Mr James Royal, consultant colorectal surgeon, Dr Dean Patterson, consultant cardiologist, representing Doctors For Patients UK both gave pre-recorded online talks.
The event was followed by a Round Table discussion followed by questions from the audience.
All of the People’s Vaccine Inquiry statements are available here: https://peoplesvaccineinquiry.co.uk/statements/
Caroline Pover and Dr Christian Buckland
Caroline shared her personal reflections on the Module 4 public hearings of the UK Covid Inquiry. She expressed her disappointment with the media's response, particularly the BBC, who seemed uninterested in her story. Other corporate media outlets provided coverage from Kate Scott on behalf of the Vaccine Injured Bereaved UK and Ruth O'Rafferty (on behalf of the Scottish Vaccine Injury Group), but Pover observed that the questioning style and content differed significantly, raising concerns about the Inquiry's independence. The lead counsel, Hugo Keith KC, displayed controlling and derogatory behaviour, using leading questions that hindered the witnesses' ability to speak freely. Incredibly, the Covid Inquiry seemed to assume the covid vaccines were not to be questioned and that witnesses were not allowed to ask questions.
Similarly the inquiry caused distress to UKCVFamily members, who felt that their legitimate questions were not being asked. Caroline explained that all questions had to be submitted in advance and many of their barrister’s questions had been rejected by the Inquiry, giving the false impression that UKCVFamily were happy with the evidence presented. The concluding message was that the Covid Inquiry was not a trial and that no one would be held responsible for the harm caused by the vaccines. Instead, the Covid Inquiry had three goals:
Increasing the UK's capacity to run clinical trials
Increasing vaccine manufacturing capacity and
Increasing the number of people getting vaccinated.
Caroline was also joined in her discussion by Dr Christian Buckland, a psychologist and psychotherapist, who commented on the total lack of coverage in the public inquiry of the issue of informed consent, which should be so fundamental to all medical treatments. Christian provides psychological support to the PVI and observed first hand the distress which the lack of proper questioning caused to the UKCVFamily members during the 3 weeks.
Caroline Pover also mentioned Brianne Dressen, a US citizen who participated in AstraZeneca's clinical trial and has since filed a case in the USA on behalf of multiple severely injured recipients. She noted that the Covid Inquiry was not interested in hearing about adverse reactions to the vaccine. Caroline Pover has written a heart-wrenching account of Brianne Dressen’s story, which will be covered in an upcoming article by HART.
Dr Jonathan Engler
Jonathan set the scene of corruption at all levels for this inquiry. He stated that the UK Covid Inquiry's Module 4 was not interested in hearing the full truth about covid vaccines. The Inquiry's framing was established from the outset, with Baroness Hallett and Hugo Keith emphasising that the Inquiry should not be used to spread "anti-vaccine misinformation or disinformation." To add fuel to the corrupt Covid Inquiry out-of-control fire, the Inquiry instead allowed many false assertions to go unchallenged.
Module 4 was characterized by
Framing to fit the official narrative
Obfuscation of uncomfortable information
Promulgation of misleading information
Whitewash with ‘limited hangout’
For instance, using illustrative quotes, Baroness Hallet before the impact video said the following: “First the film is not evidence, second it is not intended to be indicative of the experience of the vaccinated population of the UK, and third it does NOT reflect my views”
Hugo Keith before the impact video said this: “In the public interest it’s important that I seek to emphasize that the reference in this video to the obvious and well known fact that in VERY rare cases vaccination has serious side effects, must not be used as a platform to seek to undermine the vital public health role that vaccination plays in keeping people safe from disease. Or to try to [seek to] argue that at a population level vaccination is not overwhelmingly beneficial”.
His opening statement continues: “Given the many successes of the vaccine and therapeutics programme…undoubted success of the programmes…you may conclude that…” Hugo Keith KC, at the beginning of his cross-examination of Charlet Crichton…UKCVFamily members, said “it is very difficult to find out, whether [their injury/death] was causatively connected to the vaccine, was coincidental or was connected to the Covid virus”.
In essence, the Inquiry presented several misleading or false claims as facts, such as the success of the covid vaccine rollout, the idea that all vaccines are a net good for the population, and the claim that covid vaccines saved millions of lives worldwide! Other claims include the idea that covid vaccines broke the link between infection and severe outcomes, that pandemics can only be overcome with mass vaccination and that the covid vaccines were the only way out of lockdown restrictions. The real nail in the coffin of any hope of a fair inquiry was cemented by the fact that it downplayed the risks of serious side effects and deaths, describing them as “rare or very rare”, and that vaccine hesitancy was a problem that needed to be solved.
The structure of the Inquiry and the parameters for questioning core participants were designed to promote a curated story around the covid vaccines, minimising criticism and affirming the programme's success. Crucially, the vaccine-injured and bereaved groups were prevented from presenting their concerns about vaccine safety because they are critical of “the science” and that such a discussion is not relevant to the Covid Inquiry. The issues of hidden safety signals, differences in the manufacturing process, and unaddressed post-rollout safety signals were ignored.
Ruth O'Rafferty, who gave evidence on behalf of the Scottish Vaccine Injury Group, and had to give up her job because of her injuries from the vaccine was totally silenced. Hugo Keith told her what she was allowed to say and he said as she was not an expert witness she could not discuss scientific studies, and these matters would not be touched upon when she was questioned. The AstraZeneca representative was not cross-examined by any of the Inquiry Counsels, with no reason given for this omission. [Caroline Pover pointed out that all their barrister’s proposed questions for AstraZeneca were rejected by the Inquiry]
It should be emphasized that the entire Covid Inquiry was terribly upsetting for all of the vaccine injured and bereaved, as their testimonies and evidence has been totally maligned and misrepresented ⎼ almost as though vaccine injuries are an ‘abstract concept’.
Dr Elizabeth Evans
Dr Evans emphasised the failure of the UK Covid Inquiry’s Module 4 to address fundamental questions about the ethics of the covid vaccine rollout, which is arguably the biggest avoidable public health disaster in human history. To summarise, the vaccine rollout egregiously violated medical ethics, as well as the principles of equal value and dignity of every person, along with body autonomy and the protection of vulnerable patients from abuse. All medical interventions carry a risk of harm, and there is a duty to act with care and proportionality, using a patient-centred model, obtaining informed consent, and maintaining privacy and confidentiality. All of these ethical codes were violated in the covid vaccine rollout. The failure to implement the precautionary principle was staggering and based on 2 months of safety data using a novel, untested gene-based therapy. Dr Evans challenged the claim that "we had no choice" due to the threat from covid, but the decisions made were unwise and unethical and no one gave valid informed consent to the vaccines due to coercive messaging, fear mongering and lies. The use of coercive measures, such as vaccine passports and mandates, crossed the line into overt medical tyranny. But one of the most disturbing themes was the persecution and censorship of doctors who voiced vaccine safety concerns - such silencing undermines patient safety. Covid policies have set a dangerous precedent, normalising the unethical overreach into individual healthcare decisions.
Dr Evans highlighted the following ethical failures, which are best summarised in this list below.
Medical ethics are non-negotiable ⎼ they can’t be discarded in emergency for the ‘greater good’
Absence of ethical considerations in decision making and policies
Precautionary Principle disregarded ⎼ insufficient safety data, use of experimental products in pregnant women and children
Reckless rollout to whole population ⎼ regardless of covid risk
No one gave valid informed consent ⎼ use of fear and coercion
Vaccine mandates violated informed consent & medical choice
Maximising ‘vaccine confidence’ and minimising ‘vaccine hesitancy’ prioritised over ethical duty to establish vaccine safety
Doctors prevented from acting in their patient’s best interest ⎼ “One-size-fits-all”
MHRA failed to act on Yellow Card safety signals
Failure to institute a rigorous most-marketing safety surveillance system
Vaccine Damage Payment Scheme unfit for purpose
The following points were listed as the minimum information needed for obtaining valid informed consent
Temporary Emergency Use Authorization
Manufacturers immunity from liability for harm
Novel gene-based technology
Phase 3 safety trials not complete
Limited short-term safety data
No long-term safety data ⎼ cancers, fertility, antibody enhanced disease (ADE), autoimmunity
Known potential risks ⎼ clots, Vaccine-Induced Thrombotic Thrombocytopaenia (VITT), myocarditis, Guillain-Barré syndrome, neurological disorders, anaphylaxis, cardiac events, deaths
Adverse event reporting data ⎼ VAERS, Yellow Card
Vaccine immunity short-lived
Need for repeated boosters indefinitely
Does not prevent infection or transmission
Quantified individual risk from Covid
Pre-existing medical conditions not represented in trials
Naturally occurring immunity cannot be improved on
Alternatives to vaccination ⎼ available Covid treatments
Dr Ros Jones
Dr Ros Jones, a retired pediatrician, exposed the well known but startling fact that there was no justification for covid vaccination of children. Dr Jones and her colleagues at the Children’s Covid Vaccine Advisory Council (CCVAC) had sent numerous letters to regulators and politicians expressing their concerns, but their statements were not used in the inquiry and they were instead dismissed as part of the "misinformation brigade." This is exemplified by the fact that CCVAC’s first fully referenced letter was passed by Chris Whitty’s department to the Counter Disinformation Unit, more associated with monitoring for online child pornography and terrorism!
The Ethics
School closures, masks, etc.
‘Don’t kill your granny’
Vaccine as route back to normal
Turning to ethics, she pointed out how the government's measures during 2020 caused disproportionate harm to children and pump-primed their parents to accept the vaccines as the ‘route back to normal’. The risk-benefit balance of the vaccine varied widely by age, making a one-size-fits-all approach completely inappropriate and in fact harmful. Matt Hancock and Kate Bingham initially stated that the vaccine was intended for adults with comorbidities over the age of 50, but the vaccine rollout eventually included children. The MHRA authorised the use of the Pfizer vaccine for 12⎼15-year-olds based on a study of only 1,131 vaccinated children followed for 2 months, which Dr Jones argued was not a sufficient measure of safety.
The approval process
June 21: MHRA authorized - Pfizer data only
July 21: JCVI - not for healthy <18s
Aug 21: JCVI recalled - not for <16s
Sept 21: CMOs - yes for 1215s to improve mental health!
The Joint Committee on Vaccination and Immunisation (JCVI) initially decided not to recommend the vaccine for healthy children under 18, but modified their decision 48 hours later after an emergency meeting requested by the Chief Medical Officer, Chris Whitty, to allow vaccination of 16- to 17-year-olds.
Myocarditis has been acknowledged as a potential side effect of the vaccine and is now shown on the public information leaflet. In an unbelievable fabrication of the facts, the MHRA’s so-called expert misquoted the Oxford study, saying it showed more myocarditis with covid than with the vaccine - in fact the study quoted showed that for males under 40 the vaccines were associated with 6x greater risk of myocarditis than SARS-CoV-2 infection itself! Dr Jones highlighted studies from Israel and Thailand demonstrating that myocarditis was not “very rare” as claimed, with rates of 1 in 6,230 when using a passive reporting system but 1 in 29 when doing a prospective study with blood tests and diary cards.
As for the label 'mild and gets better quickly', US Teenagers hospitalised with transient chest pain and investigated with cardiac MRI scans revealed that 89% had abnormalities suggestive of heart muscle scarring and tt follow-up, 60% of these abnormal scan findings persisted.
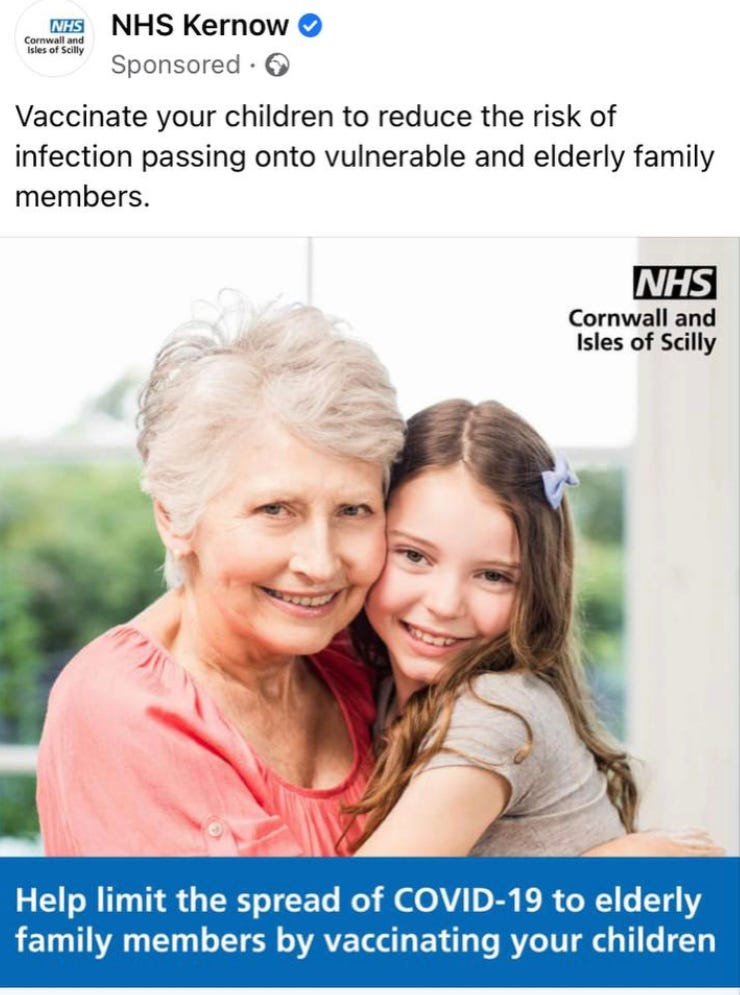
Finally, the use of incentives to get the vaccine, such as football tickets and cash offers, is not in line with informed consent procedures. Also several of the advertisements breached the principle of only allowing treatments for a child’s personal health benefit. The NHS used a gigantic direct-to-consumer advertising campaign on all platforms to encourage vaccination: “Help limit the spread of COVID-19 to elderly family members by vaccinating your children” - despite knowing transmission was not affected by the vaccines and also dissolving medical ethics to potentially harm a child with an experimental injection when their personal chances of serious health issues from the ‘virus’ was negligible.
Dr Clare Craig
Dr Clare Craig, Co-Chair of the HART group, summarised the Illusion of Benefit.
There was a deliberate exclusion of any narrative that challenged the government policies or evidence. Lead counsel, Hugo Keith, interrupted speakers and made it clear that the predetermined position would not be challenged. Claims such as "life-saving benefits" were the flavour of the Covid Inquiry without providing evidence. The vaccines' efficacy and safety were not scrutinised and the Inquiry relied on models and statistical illusions to support their claims. The vaccine's suppression of immunity for 2 weeks triggered infections earlier in susceptible people. Because of this situation, the statistical illusion was perpetuated by labelling the 2-week window after vaccination as "unvaccinated." The key point here is that by labelling those who got infections in the first 2 weeks following vaccination as infections in the “unvaccinated category,” it appeared as if the unvaccinated were at a higher risk of covid infections, while simultaneously falsely making the vaccine appear safer than it was.
The covid vaccine narrative soon shifted from reducing infections to preventing severe disease and death. Yet, real-world evidence showed that the vaccines did not reduce infections in 2021. The Imperial College model that claimed the vaccines saved over 14 million lives globally and helped prevent Long Covid, were nothing more than unscientific and worthless modelling. Real-world evidence showed that populations in the USA and Europe (except UK, Portugal, and Ireland) saw no benefit from vaccines in 2021.
Representatives from AstraZeneca, Pfizer and Moderna were questioned during the Covid Inquiry. Unbelievably, Dr. Justin Green from AstraZeneca claimed that on the basis of a single death in the trial placebo group, this was sufficient grounds to indicate an "excellent product.” Even the US trial safety board condemned the "misleading" press releases quoting 100% effectiveness on the basis of one death in the placebo arm, as incorrect. But no one at the Covid Inquiry challenged Dr. Green’s assertion. The Moderna representative, Mr. Darius Hughes, denied any suspected unexpected serious adverse reactions during the trials. To illustrate the obfuscation, other mentions of clinical trials were forbidden during the inquiry.
Suppression of dissenting voices was rife in the Inquiry. Anyone who was critical of vaccine safety and trial data, were interrupted by counsel Hugo Keith. He dismissed discussions on the differences between trial and mass-produced vaccine products, as well as vaccine injuries in trials, along with regulatory failures. He claimed there was no time to delve into such topics. The Inquiry also avoided discussing several key topics, including lipid nanoparticle risks, cardiac risks and sudden death, spike protein production, and differences in doses between Pfizer and Moderna vaccines.
Despite the use of the word “rare” over 130 times in the Inquiry, data showed unequivocally that excess deaths, working-age disabilities and heart disease increased significantly after the Spring of 2021. Trial data revealed a 1 in 800 risk of serious adverse events for mRNA vaccines and 1 in 550 for Pfizer, and that the mass-produced Pfizer vaccine had 2⎼13 times more adverse reactions than the laboratory version used in the clinical trials. Dr Craig criticised the Covid Inquiry for idolizing the vaccine narrative, silencing dissenting voices, and refusing to question the myths surrounding the covid pandemic and vaccine effectiveness. In a statement to The Epoch Times, Dr Craig said the complexity of the science behind the vaccines is perfectly possible for barristers to understand and that questions being asked of expert witnesses are a deliberate choice. “I think there’s nothing about medicine which is not accessible to people who put the time in...It’s not some kind of sacred knowledge. It’s just knowledge. “And I think that the KCs understand the issues very well, and I think that is why they navigate it the way they’re doing, because they know exactly what they don’t want to be said.”
Nick Hunt
Nick Hunt, a former Senior Civil Servant in the Ministry of Defence, went on to discuss MHRA failures. He co-authored a 36-page report documenting the harms caused by covid vaccines, and the MHRA cataclysmic failures in safety management of medicines. Hunt also co-authored a Witness Statement to the Covid Inquiry, but guess what…he was not called to present their evidence. MHRA’s slow response to safety issues for medicines in general ⎼ taking an average of 11 years before a medicine is withdrawn from the market on the basis of safety grounds ⎼ is appalling. June Raine, the head of MHRA, admitted in her Written Evidence that the agency does not investigate all Yellow Card reports, even fatal ones. Instead it relies on statistical analysis of the whole Yellow Card database to generate safety signals. The Inquiry also failed to ask about the lack of causation assessment in reported adverse events. Statistical analyses used by MHRA have been shown to miss safety signals. As stated earlier, the covid vaccines were mass-produced using a different process than the product used in clinical trials, with no comparative safety data. The MHRA did not include information about quality concerns, lack of comparative safety data, and consequential safety risks in its advice to Ministers recommending approval of the vaccines.
Other key issues, such as DNA contamination and batch testing, were ignored. Pfizer, Moderna and AstraZeneca were required to conduct Post-Authorisation Safety Studies, but the Inquiry did not ask about the status of these studies or the potential risks associated with the covid vaccines. The Inquiry ignored evidence that an Interim Report from Pfizer revealed higher incidences of heart conditions among the vaccinated. The MHRA withheld this report so Nick Hunt asked the inquiry why. In an extraordinary display of continued lies, June Raine denied having received such a report. The Inquiry's 'expert witness' Professor Alhambra stated he did not think that the increase in heart conditions was caused by the Pfizer vaccine.
Ultimately, Hunt explained that MHRA’s safety management is all relative. The approval of treatments is based on benefit being greater than risk (often using poor or non-existent data), and the surveillance is based on a new drug or therapy being no worse than similar ones, and with no threshold to suspend agents. Given that the covid vaccines were different to any other drugs on the market, conclusions drawn from comparisons are pointless. Perhaps more significantly, Hunt explained that MHRA is not subject to safety audits and he went on to give a number or examples of failures.
Examples of claims ignored or denied in the Covid Inquiry:
No reduction in infections - As real-word data showed transmission continued.
No clear reduction in deaths - Models claimed millions saved, but real-world mortality patterns did not reflect this
Statistical illusions - Early post-vaccination infections classified as unvaccinated, skewing results
Omicron changed the game - Less severe from the start, yet inquiry ignored it
Trial evidence?- One single claimed placebo death used to justify rollout.
MHRA failures for Covid Vaccines
Key testing omitted ⎼ no pharmacology, pharmacokinetics
Process 1 vs Process 2 ⎼ product rolled out not tested
Slow to react to AstraZeneca problems
Missed safety signals
Unaware of Coroners’ reports
Patient Information Leaflets: possibility of death not mentioned
Post Authorisation Safety Studies (PASS): significant increase in heart conditions in vaccinated cohorts
MHRA failures for Medicines in General
No investigation of Yellow Card (YC) reports ⎼ not even the fatal and serious ones
No assessment of causation
Missing information from YCs ⎼ batch, age of subject, time from admission
Slow to react ⎼ average 11 years to withdraw drugs on safety grounds
Manpower shortages
Key differences to other safety critical sectors
No threshold of safety ⎼ no criteria for numbers of death/injury before vaccine
No independent safety audit
No personal accountability ⎼ MHRA decisions by groups not individuals
Myths
“Side effects are rare”
“Millions of lives saved”
Mr Hunt quoted Patrick Vallance’s 2014 statement “In the future medicines will come to market quicker with less data, with more research being conducted in the post-license phase". Nick ended his talk with the stark warning that unless the MHRA's safety management is completely reformed, medicine safety will continue to deteriorate.
Mr James Royle
James Royle is a colorectal surgeon working in North East England. He explained in a recorded interview that when lockdowns were announced in March 2020, he continued working in the local hospital but was never overwhelmed with patients. He believed early on this was a pandemic of fear, and knew his personal risk was low, so felt natural immunity was sufficient. In October 2020, only cancer emergency clinics continued, other assessments were by telephone. He was perturbed by where all emergency operations were going, as most of appendicitis, inflamed gallbladders, and diverticulitis were being managed in the community. Lockdown was a devastating failure and he warned it would not be effective and would cause harm. The detrimental impact to patients was obvious, because being isolated and housebound with incessant terrifying media messaging generated huge anxiety and fear. The lack of fresh air, sunlight, and exercise, led to immunosuppression and vitamin D deficiency collectively adding to poor outcomes. It was no surprise to him that the elective cancer mortality rate went from one death in his first 5 years as a consultant to six mortalities within 30 days, five from non covid and three of these from sudden cardiac deaths.
The ‘only way out of the pandemic’ was the coerced so-called vaccines that soon became a one-size-fits-all. He wanted to stop vaccines in healthy children and he was skeptical from the start of the vaccine rollout of these untested gene-therapy injections. From around March 2021, he noticed new patterns of disease he had never seen before in his patients. The first was blood clotting, with CT scans were showing multiple pulmonary thrombosis, clots in the pulmonary vasculature that were not typical pulmonary emboli. Also venous thromboses, clots unlike anything he had seen before and affecting the same three vessels: portal vein, the superior mesenteric vein and the splenic vein. These patients were typically middle aged (31 to 77 years) presented with abdominal pain and no prior pathology or classical risk factors. He was also seeing cases of ischaemic bowel, likely caused by micro clotting. These thrombotic cases were positive for VITT following the AstraZeneca vaccine, but also occurred after mRNA shots. The spike protein has been found in many organs following vaccination. Some patients presented with extensive pancreatic necrosis. He observed sudden deaths from necrotizing pancreatitis in elderly patients following the vaccine boosters. There was also a noticeable increase in appendix cancers and pancreatic cancers.
Following the vaccine rollout there has been an alarming and significant increase in cancers in all countries, including colorectal cancers. These cancers have been termed colloquially as “turbo cancers” observed by the public as well as clinicians. Despite mainstream narratives to the contrary, there has been a dramatic increase in cancers in 2021 very soon after the vaccine rollout. These excess cancer deaths are extremely aggressive and of a different biology, particularly among younger patients. He has noticed aggressive widespread recurrences in previously successfully treated bowel cancer patients. Many present with incurable, stage IV aggressive cancers and die within weeks or months. In his past experience, most sporadic cancers are operable when diagnosed but these new cases are highly aggressive. All his colleagues are reporting changes in the patterns and incidences in the past 2⎼3 years.
Postulated causes such as inherited or genetic cancers are unlikely as no such mutations are identified. Poor diet, ultra processed foods and lack of exercise cannot explain the rapid changes of cancers presented. Delayed diagnosis or missed cancers owing to the temporary halt to screening programmes does not explain the rapid cancer rise. His clinic still screened and treated patients for all but a few weeks in early 2020, and in any case the rise in cancers in 25⎼40 year-olds is in an age group not eligible for screening. Plasmid contamination, presence of SV40 tumour promoter and disruption of p53 tumour suppressor explains the rise in cancers observed. He submitted 20 Yellow Card Reports but the MHRA ignored the data, and gave no indication they are analysing such data.
He concluded that the Covid vaccines are neither effective or safe, and he demands that these injections be stopped with immediate effect.
Professor Angus Dalgleish
Professor Angus Dalgleish discussed the cancer increases following the booster vaccine rollout, as well as top-line key takehomes about innate and adaptive immunity. He mentioned two key peer-reviewed papers, which predicted that the vaccine rollout would be nothing short of a catastrophe, especially because of the warning signs of the science behind the therapy.
In particular, in the first paper he and his co-authors pointed out that the spike protein in SARS-CoV-2 was highly positively charged (this was part of his contention that it must have been manipulated in a laboratory) and also that it showed 78.4% similarity with human-like epitopes. The similarity to human proteins has two potential problems, firstly failure to provide protection as it’s too similar to create a strong response and secondly the likelihood of inducing autoimmune disease or antibody-dependent enhancements. These concerns have indeed been shown to be the case.
Professor Dalgleish explained that this 78% homology with human epitopes, especially PF4 (platelet factor 4, a small cytokine released from clotting cells upon platelet activation), meant that clotting and platelet dysfunction were predictable from this data early on. The myelin homology within the sequences present in the vaccines (myelin is that fatty sheath which coats nerves) would also be predictive of neurological problems such as transverse myelitis, Bell's Palsy and Guillain-Barré Syndrome. Indeed, these conditions are on the MHRA website as side effects! Requests to exclude these regions from any vaccines were ignored by SAGE and the Chief Medical Officer (Professor Chris Whitty) and Chief Scientific Officer (Professor Patrick Vallance).
His second paper was about the history of coronavirus vaccines which have never been successful, partly because often the experimental animals died of enhanced infection. And partly because coronaviruses mutate rapidly so any vaccine is out-of-date before it is given. But the recipients will still make antibodies to the original vaccine strain instead of to the new variants.
mRNA and unwanted effects
Professor Dalgleish explained how mRNA vaccines can increase cancers. He had not originally expected increased cancer risk, but after the rollout of the boosters he started seeing aggressive relapses in his melanoma patients after 5, 10 or even 15 years in remission. A paper entitled “Evidence of exhausted lymphocytes after the third anti-SARS-CoV-2 vaccine dose in cancer patients” published in late 2022 confirmed the increased risk of immune downregulation in cancer patients.
He highlighted
Numerous reports of batch to batch variation with DNA contamination;
SV40 promoter (a known oncogenic sequence present in some previous vaccines);
mRNA vaccines cause frame-shifting and unwanted genetic instructions;
They are not rapidly cleared as claimed, but can persist for over a year and have been detected in every organ at autopsy and in cancers removed by surgery.
The mRNA spike proteins from the vaccine bind to known tumour suppressor genes, such as p53, BRCA, and MSH-3, which suppress cancer activity but when mutated greatly increase early cancer risk. The long-lived spike protein can cause chronic inflammation and chronic clotting, and abnormal clotting is recognised as a major progression factor in cancer, especially pancreatic and prostate cancer.
He ended by rather depressingly saying he thought we were only just seeing the beginning of this, with cancers likely to take several years to manifest themselves.
Dr Dean Patterson
Dr Dean Patterson, a consultant cardiologist from Guernsey, spoke on behalf of the Doctors For Patients UK, explaining that he wanted to shine a light on those who had been harmed by the Covid injections. He started with some of the basic science (or lack of) involved in these new gene-based vaccines. The Covid vaccines produce a secondary product ⎼ namely they provide the genetic instructions to make the viral spike protein de novo ⎼ and this product lingers in the body and is widely distributed and does not stay in the injection site, as originally claimed. The biodistribution of the vaccine contents were never profiled and contaminants from the LNP and genetic manufacturing process all contributed to the lack of known data about these products and certainly cast doubt over their safety. The presence of the oncogenic SV40 promoter, as well as suppression of p53 tumour suppressor are particularly concerning. Signals are beginning to come through about increased cancers in recipients of the Covid vaccine.
Dr Patterson then turned to cardiac problems and described seeing patients with nonbacterial thrombotic endocarditis. This is a rare condition but he started to see patients presenting with this in 2021 following the rollout of the vaccines. He highlighted the disruption to the endothelial lining of the heart and blood vessels leading to abnormal clotting. He showed a slide including a list from the FDA from October 2020 of the “adverse events of special interest”.

The discovery of large ‘rubbery clots’ in autopsies and in vaccine harmed patients were all too evident, along with encephalitis. Guillain-Barré Syndrome, myocarditis, strokes, and thrombosis seen in many patients. Even young, previously fit 20-year-olds were coming to his clinic and presenting with symptoms of acute myocardial infarction, which was unprecedented before 2021, and was only seen in individuals who had received a Covid vaccine. Full investigation showed they in reality had myocarditis. Dr Patterson suggested that for older patients presenting with chest pain, a diagnosis of an acute heart attack would be made and the underlying myocarditis would easily be missed. He explained that there is an overlap, such that people with some pre-existing heart disease could deteriorate rapidly if they developed myocarditis.
Dr Patterson also reported patients developing severe rashes within 18 hours of the vaccine who then went on to experience severe chest pain. The safety signals of this spectrum of cardiac events, especially in young patients, was an all too clear indicator that the vaccines were wreaking havoc. Patients were often discharged in the early period of the pandemic and told their symptoms were caused by stress. Notably, following the vaccine campaign, it was becoming clear a trend was emerging for a wide range and distribution of cardiac events nationally (and globally), but formal monitoring of these warning signals was never undertaken.
Dr Jonathan Engler
Dr Engler closed the meeting by reminding everyone of the overall aims of the People’s Vaccine Inquiry, namely:
Immediate cessation of the use of mRNA products as vaccines
Reform of the Yellow Card system which is not fit for purpose
Reform of the Vaccine Damage Payment Scheme (VDPS) which is grossly unfair
For manufacturers – rather than taxpayers – to be liable for the huge amount of harm caused
Stop revolving door between regulators and Industry which creates implicit conflicts of interest
Place power of medical decision-making back to individual
So grateful there are some wonderful people working so hard to try and right the wrongs. We must not let this go. You will be vindicated.
Fantastic article, I think this whole episode is being buried deeper and deeper by the state and those responsible. Surely history will uncover the truth at some point. I'm so grateful for people that have even the limited exposure that can highlight the injustices and downright scandal that is being whitewashed.