
Concerns over the covid mRNA injections keep coming
Study suggests spike protein production persists for at least several months in 50% of subjects


One of the most egregious missteps (a word which might be construed as generous) by drug regulators around the world was to allow the MRNA injections to proceed through a pathway reserved for the class of products termed vaccines.
This classification allowed them to skip certain areas of study prior to rollout, for example carcinogenicity and biodistribution (the elucidation of where the injected product ends up in the body), on the basis that “vaccines are broken down at the injection site”.
In fact, that assumption - that the product gets broken down at the injection site - was repeatedly promoted by the companies themselves, major drug regulators, and the proponents of the injections generally.
Yet it is false, and has always been known to be false.
A biodistribution study in rats, a report of which was prised out of the FDA as part of the litigation spear-headed by Aaron Siri (FDA / Pfizer had wanted the data hidden for 75 years) showed that the product was widely distributed throughout the body after injection, and the regulators must have known this, while they were insisting to the public that this was not the case. (See thread here.)
The carrier of the mRNA - the lipid nanoparticles - was developed with a view to use to convey cancer drugs to their target; as such, it is specifically designed to pass through various membranes in the body and become widely distributed.
In fact, a recent paper touted the ability of LNPs to cross the “blood brain barrier” (which is an evolved physical membranous barrier designed to protect our ultra-delicate neurological tissue from a variety of pathogens and toxins) as something which would be useful for treating neurological diseases. The authors of that paper were clearly oblivious to the dangers that mRNA carried in the LNPs might - after crossing the blood brain barrier - transfect the brain, marking those cells out for destruction by the immune system.
Another big unknown is: for how long does the spike protein production continue?
An optimal design for these products (to the extent that such a thing is possible) would ensure that the spike protein production only continued for a very short time, long enough for the immune system to mount an antibody response. That is basically hours, or a day or two at most.
The production should then switch off, because:
The spike protein itself is thought to have a variety of toxic effects, including on the heart.
Cells which are producing it on their surface get marked for destruction by the immune system, resulting in the potential for a variety of ill-effects, especially of an auto-immune and / or inflammatory nature.
Continued production of spike protein may have other undesirable effects on the immune system in general, or in terms of its response to similar coronaviruses.
The covid vaccine enthusiasts like to conflate “spike from infection” with “spike from vaccine”, explaining away all adverse events as being caused by viral infection. However, this is a false equivalence for a number of reasons, which can be summarised thus:
It is unreasonable to equate the presence of a viral protein in low quantities, for a short period of time, handled by the respiratory mucosal immune mechanisms very efficiently in nearly everyone, to the injecting of an instruction for the body to create that substance throughout every organ system in uncontrollable locations and amounts and for an unknown duration of time.
The spike protein created by the vaccine in any way differs in a number of ways from the “Wuhan spike”; the functional implications of such differences are unknown.
In a paper published recently, Italian researchers utilised a key difference between vax-spike and “Wuhan-spike” to try to start answering the thorny question: for how long is spike protein produced?
One of the major differences between the spike protein produced by all the vaccines and the “Wuhan spike” is known as a “2P substitution” whereby at 2 positions the amino acids are replaced by another amino acid, proline. There’s quite a straightforward (though rather biased) explanation of it here.
(As an aside, the “2P substitution” is subject to a patent filed in 2016, colloquially known as the “070 patent”. This article explores some peculiarities around it, including the fact that Moderna seem to be in breach of the patent but the US government - one of the patent’s co-owners - has not taken any action.)
The 2P substitution is designed to increase the effectiveness of the vaccine by stabilising the spike protein. It is, of course, arguable whether any efficacy has been demonstrated at all, but that is irrelevant to the point we are making here.
The notable point is that this biochemical manipulation is actually easily detectable by a test using mass spectrometry; it is, therefore, possible to distinguish with certainty between natural “Wuhan spike” from infection, and that created as a result of mRNA injection.
In the Italian study, 60 healthy care workers were recruited across these three groups:
20 who had received 2 doses of mRNA vaccine
20 unvaccinated and covid uninfected individuals (no antibodies and negative PCR)
20 unvaccinated persons that had had COVID-19
The key result is below:
The specific PP-Spike fragment was found in 50% of the biological sample analyzed (Figures 1C–E and 2).
This presence was independent of the SARS-CoV-2 IgG antibody titer.
The minimum time PP-Spike was detected was 69 days after vaccination, while the maximum time was 187 days.
All controls (samples from unvaccinated individuals) were negative.
The control group (20 unvaccinated people) was also tested after contracting COVID-19 and was negative for PP-spike.
NB: The article doesn’t explicitly say what the “biological samples” actually were, though a passage describing the blood collection technique used strongly implies these were all blood samples.
The results can be read as highly suggestive that the spike protein is being created for an extended time in the vaccinated - and ONLY in the vaccinated. The data suggests that this is happening in around half the individuals injected with these substances.
It should be noted that the range of 69 to 187 days was the range of sampling times after vaccination. We don’t know what repeat samples at later time points would have shown. It certainly cannot be ruled out that spike protein production continues well beyond the sampling time point, possibly indefinitely.
It has been suggested by some that as the mass spectrometry is only detecting a very small fragment of the spike protein, it’s possible that the entire protein is not present - but rather this is evidence of the immune system presenting parts of the protein (ie in this case the part containing the 2P substitution) as part of its normal processes which last for some time.
However, and especially in the presence of other disturbing safety signals, the onus is on those who make those assertions to provide proof. We are long past the point where those with legitimate concerns triggered by a seemingly never ending tidal wave of incoming safety signals should have to prove anything, let alone formulate a detailed mechanism for harm.
In any case, another study, published at around the same time as the above, strongly supports the idea that spike protein is being created longer-term.
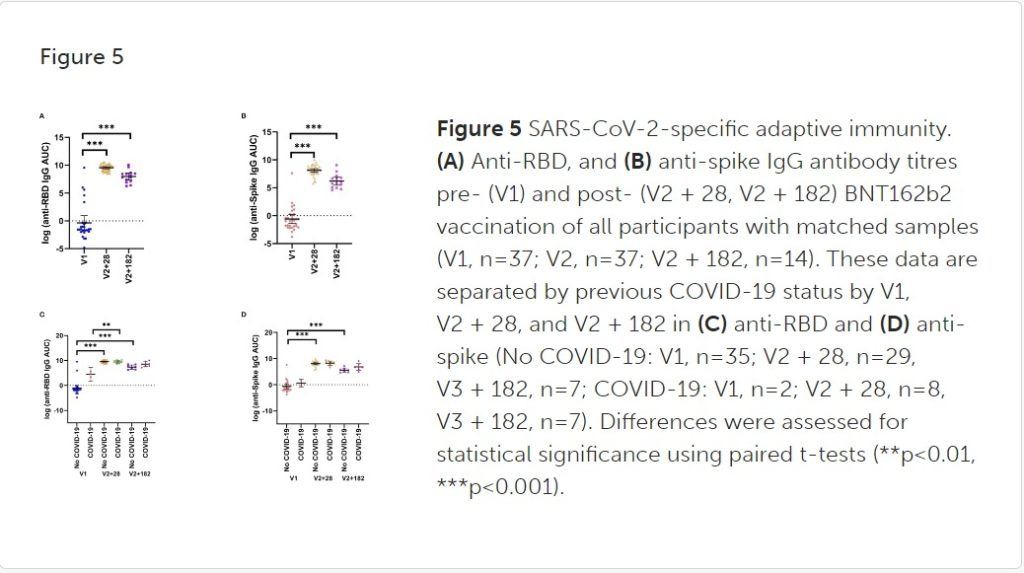
In this study a group of Australian researchers performed a range of measurements on blood samples taken from 29 children, aged 5-11 years, before and 28 days after a second BNT162b2 vaccination were analysed. Samples from eight children were analysed six months after BNT162b2 vaccination.
The tests performed indicated some profound changes in the strength of cytokine responses to a wide range of viral and bacterial pathogens on which we won’t comment further here, but for present purposes the most interesting - and concerning finding - was that anti-spike antibodies remained significantly elevated in all the samples taken 6 months after vaccination (see A and B in the below).
Since - ordinarily - antibodies decline rapidly after a new antigen is presented transiently to the immune system, this high rate of antibodies present so long after injection is difficult to explain in any other way than that the antigen - ie the spike protein - is being made for an extended period.
These papers on their own should result in an immediate suspension of these products, but then so also should have the hundreds of other papers and worrying data points generated during the ghastly experiment of the past few years.
Hence, and very unfortunately, it is most likely that nothing at all will happen.
Igor Chudhov has written an excellent blog post on this study which can be found here.
I am reminded of the George Orwell quote "The party told you to reject the evidence of your eyes and ears. It was their final most essential command". I read and hear about the damage from the covid vaccines and I have seen it with my own eyes, I hear their life altering stories and I refuse to reject the evidence. The government can spew their propaganda but I will not believe or listen to it.
Clearly we can identify the presence of spike protein derived from the “shot” (as distinct from that from the virus) in endovascular lesions causing fatal MI’s , and I know this has been done in at least one autopsy study in Germany. But wouldn’t it also be possible to identify the culprit in non fatal events( such as MI or stroke) from biopsies ? Sudden and potentially fatal events in the heart and brain are dramatic , but there must surely be evidence of vascular lesions in many other organs. Surely it would be possible to recruit a few pathologists to look at this.